Alhossain A Khalafallah, Abdul-Rauf O Ibraheem, Qiong Yue Teo, Abdul-Majeed Albarzan, Ramanathan Parameswaran, Emily Hooper, Toly Pavlov, Amanda E Dennis, Terry Hannan
{"title":"Review of Management and Outcomes in Women with Thrombophilia Risk during Pregnancy at a Single Institution.","authors":"Alhossain A Khalafallah, Abdul-Rauf O Ibraheem, Qiong Yue Teo, Abdul-Majeed Albarzan, Ramanathan Parameswaran, Emily Hooper, Toly Pavlov, Amanda E Dennis, Terry Hannan","doi":"10.1155/2014/381826","DOIUrl":null,"url":null,"abstract":"<p><p>Pregnancy is a hypercoagulable state associated with an increased risk of venous thromboembolic disease (VTE). We retrospectively studied 38 Caucasian pregnant women with thrombophilia risk and compared their obstetric outcomes with a matched cohort without known thrombophilia risk during the period between January 2007 and December 2010. There were (2) cases with factor V Leiden, (6) prothrombin gene mutation, (1) antithrombin III deficiency, (2) protein C deficiency, (3) protein S deficiency, (10) MTHFR mutation, (7) anti-cardiolipin antibodies, and (1) lupus anticoagulant. Patients without thrombophilia who presented with recurrent unprovoked VTE were considered as high risk (6 cases). Most patients received anticoagulation (34/38) with aspirin only (6), enoxaparin (27), and warfarin (1). Twenty-six out of thirty-eight pregnant women (68.4%) with an increased risk of thrombophilia experienced one or more obstetric complications defined as hypertension, preeclampsia, placenta abruptio, VTE, and oligohydramnios, compared with 15 out of 40 (37.5%) pregnant women in the control group (OR 3.6; 95% CI 1.42, 9.21, P < 0.001). The incidence of obstetric complications was significantly higher in the thrombophilia group compared to the controls. However, these complications were the lowest among patients who received full-dose anticoagulation. Our study suggests that strict application of anticoagulation therapy for thrombophilia of pregnancy is associated with an improved pregnancy outcome. The study was registered in the Australian and New Zealand Clinical Trials Registry under ACTRN12612001094864. </p>","PeriodicalId":73520,"journal":{"name":"ISRN obstetrics and gynecology","volume":"2014 ","pages":"381826"},"PeriodicalIF":0.0000,"publicationDate":"2014-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/381826","citationCount":"15","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ISRN obstetrics and gynecology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/381826","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 15
Abstract
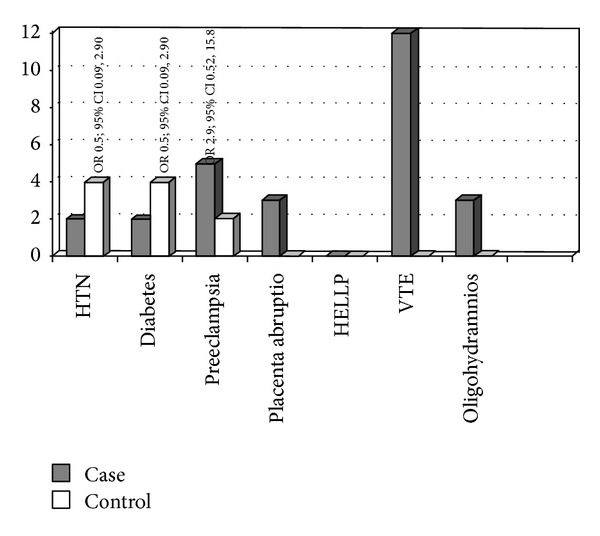
Pregnancy is a hypercoagulable state associated with an increased risk of venous thromboembolic disease (VTE). We retrospectively studied 38 Caucasian pregnant women with thrombophilia risk and compared their obstetric outcomes with a matched cohort without known thrombophilia risk during the period between January 2007 and December 2010. There were (2) cases with factor V Leiden, (6) prothrombin gene mutation, (1) antithrombin III deficiency, (2) protein C deficiency, (3) protein S deficiency, (10) MTHFR mutation, (7) anti-cardiolipin antibodies, and (1) lupus anticoagulant. Patients without thrombophilia who presented with recurrent unprovoked VTE were considered as high risk (6 cases). Most patients received anticoagulation (34/38) with aspirin only (6), enoxaparin (27), and warfarin (1). Twenty-six out of thirty-eight pregnant women (68.4%) with an increased risk of thrombophilia experienced one or more obstetric complications defined as hypertension, preeclampsia, placenta abruptio, VTE, and oligohydramnios, compared with 15 out of 40 (37.5%) pregnant women in the control group (OR 3.6; 95% CI 1.42, 9.21, P < 0.001). The incidence of obstetric complications was significantly higher in the thrombophilia group compared to the controls. However, these complications were the lowest among patients who received full-dose anticoagulation. Our study suggests that strict application of anticoagulation therapy for thrombophilia of pregnancy is associated with an improved pregnancy outcome. The study was registered in the Australian and New Zealand Clinical Trials Registry under ACTRN12612001094864.
妊娠是一种与静脉血栓栓塞性疾病(VTE)风险增加相关的高凝状态。在2007年1月至2010年12月期间,我们回顾性研究了38名有血栓形成风险的高加索孕妇,并将她们的产科结果与没有血栓形成风险的匹配队列进行了比较。(2) Leiden因子V,(6)凝血酶原基因突变,(1)抗凝血酶III缺乏,(2)蛋白C缺乏,(3)蛋白S缺乏,(10)MTHFR突变,(7)抗心磷脂抗体,(1)狼疮抗凝剂。无血栓形成的患者出现复发性非诱发性静脉血栓栓塞被认为是高风险(6例)。大多数患者只接受阿司匹林(6)、依诺肝素(27)和华法林(1)的抗凝治疗(34/38)。38名血栓形成风险增加的孕妇中有26名(68.4%)经历了一种或多种产科并发症,定义为高血压、先兆子痫、胎盘早剥、静脉血栓栓塞和羊水过少,而对照组中40名孕妇中有15名(37.5%)(or 3.6;95% ci 1.42, 9.21, p < 0.001)。与对照组相比,血栓形成组的产科并发症发生率明显更高。然而,这些并发症在接受全剂量抗凝治疗的患者中是最低的。我们的研究表明,严格应用抗凝治疗妊娠血栓形成与妊娠结局的改善有关。该研究已在澳大利亚和新西兰临床试验登记处注册,编号为ACTRN12612001094864。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
