Impact of minimal residual disease, detected by flow cytometry, on outcome of myeloablative hematopoietic cell transplantation for acute lymphoblastic leukemia.
Merav Bar, Brent L Wood, Jerald P Radich, Kristine C Doney, Ann E Woolfrey, Colleen Delaney, Frederick R Appelbaum, Ted A Gooley
{"title":"Impact of minimal residual disease, detected by flow cytometry, on outcome of myeloablative hematopoietic cell transplantation for acute lymphoblastic leukemia.","authors":"Merav Bar, Brent L Wood, Jerald P Radich, Kristine C Doney, Ann E Woolfrey, Colleen Delaney, Frederick R Appelbaum, Ted A Gooley","doi":"10.1155/2014/421723","DOIUrl":null,"url":null,"abstract":"<p><p>In this retrospective study, we evaluated the impact of pre- and posttransplant minimal residual disease (MRD) detected by multiparametric flow cytometry (MFC) on outcome in 160 patients with ALL who underwent myeloablative allogeneic hematopoietic cell transplantation (HCT). MRD was defined as detection of abnormal B or T cells by MFC with no evidence of leukemia by morphology (<5% blasts in marrow) and no evidence of extramedullary disease. Among 153 patients who had pre-HCT flow data within 50 days before transplant, MRD pre-HCT increased the risk of relapse (hazard ratio (HR) = 3.64; 95% confidence interval (CI), 1.87-7.09; P = .0001) and mortality (HR = 2.39; 95% CI, 1.46-3.90, P = .0005). Three-year estimates of relapse were 17% and 38% and estimated 3-year OS was 68% and 40% for patients without and with MRD pre-HCT, respectively. 144 patients had at least one flow value post-HCT, and the risk of relapse among those with MRD was higher than that among those without MRD (HR = 7.47; 95% CI, 3.30-16.92, P < .0001). The risk of mortality was also increased (HR = 3.00; 95% CI, 1.44-6.28, P = .004). These data suggest that pre- or post-HCT MRD, as detected by MFC, is associated with an increased risk of relapse and death after myeloablative HCT for ALL. </p>","PeriodicalId":18102,"journal":{"name":"Leukemia Research and Treatment","volume":"2014 ","pages":"421723"},"PeriodicalIF":0.0000,"publicationDate":"2014-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2014/421723","citationCount":"79","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Leukemia Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2014/421723","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2014/3/23 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 79
Abstract
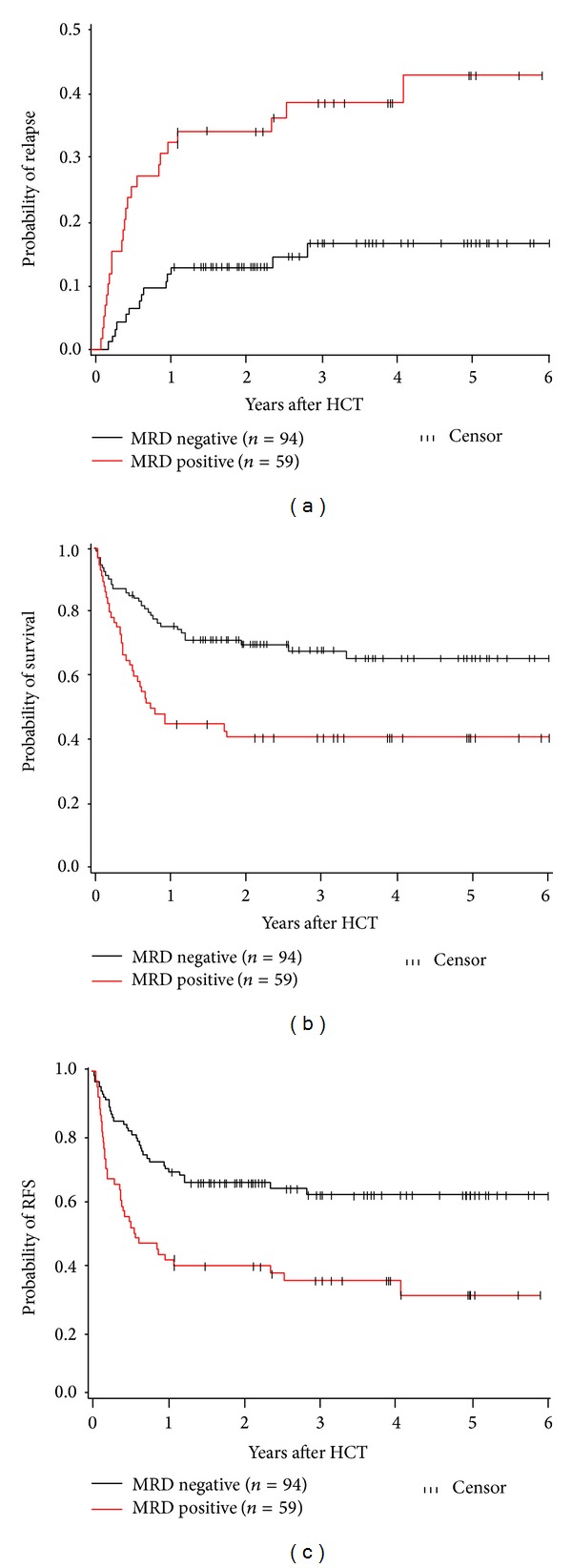
In this retrospective study, we evaluated the impact of pre- and posttransplant minimal residual disease (MRD) detected by multiparametric flow cytometry (MFC) on outcome in 160 patients with ALL who underwent myeloablative allogeneic hematopoietic cell transplantation (HCT). MRD was defined as detection of abnormal B or T cells by MFC with no evidence of leukemia by morphology (<5% blasts in marrow) and no evidence of extramedullary disease. Among 153 patients who had pre-HCT flow data within 50 days before transplant, MRD pre-HCT increased the risk of relapse (hazard ratio (HR) = 3.64; 95% confidence interval (CI), 1.87-7.09; P = .0001) and mortality (HR = 2.39; 95% CI, 1.46-3.90, P = .0005). Three-year estimates of relapse were 17% and 38% and estimated 3-year OS was 68% and 40% for patients without and with MRD pre-HCT, respectively. 144 patients had at least one flow value post-HCT, and the risk of relapse among those with MRD was higher than that among those without MRD (HR = 7.47; 95% CI, 3.30-16.92, P < .0001). The risk of mortality was also increased (HR = 3.00; 95% CI, 1.44-6.28, P = .004). These data suggest that pre- or post-HCT MRD, as detected by MFC, is associated with an increased risk of relapse and death after myeloablative HCT for ALL.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
