{"title":"Comparison of 2-Level Versus 1-Level Total Disc Replacement: Results From a Prospective FDA-Regulated Trial.","authors":"Jack E Zigler, Donna D Ohnmeiss","doi":"10.1016/SASJ-2008-0009-RR","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fusion has been the traditional surgery for painful disc degeneration unresponsive to nonoperative care. Fusion rates may decline in multilevel procedures. Also, fusion may force additional stress onto adjacent discs. This effect may be amplified in multilevel procedures. Single-level total disc replacement (TDR) has been found to be as effective as fusion. There have been few published reports addressing 2-level TDR. The purpose of this study was to compare results of TDR at 2 levels to 1-level procedures.</p><p><strong>Methods: </strong>This report included the first consecutive 86 patients who had reached 24-month follow-up from among those enrolled in the ProDisc-L investigational device exemption (IDE) study of patients undergoing TDR at 1 level (N = 54) or at 2 levels (N = 32). Clinical outcome measures included visual analog scales (VAS) assessing pain, Oswestry Disability Index, satisfaction measured by VAS, and responses to the question regarding whether the patient would have the same surgery again.</p><p><strong>Results: </strong>Operative time and length of hospitalization were significantly less in the 1-level cases compared to 2 levels (61.6 min vs 97.8 min; and 1.89 days vs 2.44 days; P < .05). There was a trend for less blood loss in single-level cases (59.0 mL vs 79.2 mL) (.05 < P < .09). VAS and Oswestry scores were significantly improved in both groups postoperatively (by approximately 50%). At no follow-up were there significant differences in VAS, Oswestry, or patient satisfaction scores between the single- and 2-level patients. At all follow-ups, the mean satisfaction in both groups was greater than 7.5 on a scale of 0 to 10.</p><p><strong>Conclusions: </strong>Patients undergoing 2-level TDR improved significantly postoperatively based on VAS and Oswestry scores, and there were no significant differences in outcome scores when comparing 1- and 2-level TDR.</p><p><strong>Clinical relevance: </strong>This study suggests that 2-level TDR can be undertaken in appropriately selected patients and achieve results similar to singlelevel cases.</p>","PeriodicalId":88695,"journal":{"name":"SAS journal","volume":"2 3","pages":"140-4"},"PeriodicalIF":0.0000,"publicationDate":"2008-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/SASJ-2008-0009-RR","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAS journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/SASJ-2008-0009-RR","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2008/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 11
Abstract
Background: Fusion has been the traditional surgery for painful disc degeneration unresponsive to nonoperative care. Fusion rates may decline in multilevel procedures. Also, fusion may force additional stress onto adjacent discs. This effect may be amplified in multilevel procedures. Single-level total disc replacement (TDR) has been found to be as effective as fusion. There have been few published reports addressing 2-level TDR. The purpose of this study was to compare results of TDR at 2 levels to 1-level procedures.
Methods: This report included the first consecutive 86 patients who had reached 24-month follow-up from among those enrolled in the ProDisc-L investigational device exemption (IDE) study of patients undergoing TDR at 1 level (N = 54) or at 2 levels (N = 32). Clinical outcome measures included visual analog scales (VAS) assessing pain, Oswestry Disability Index, satisfaction measured by VAS, and responses to the question regarding whether the patient would have the same surgery again.
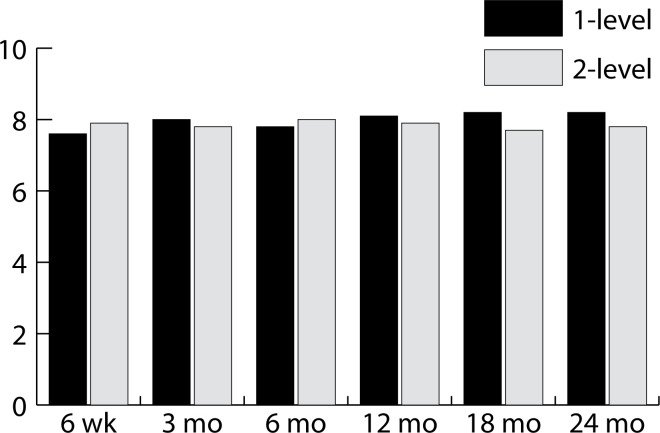
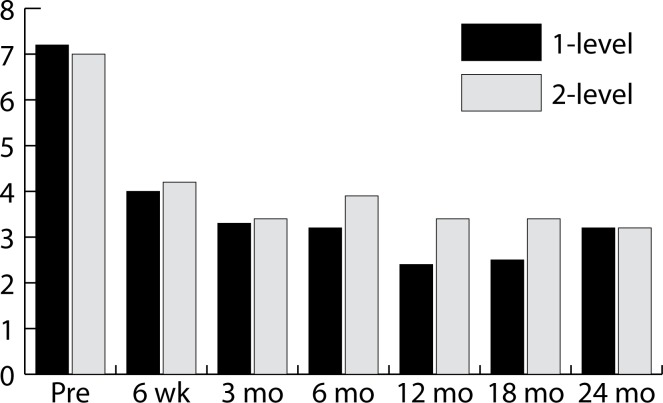
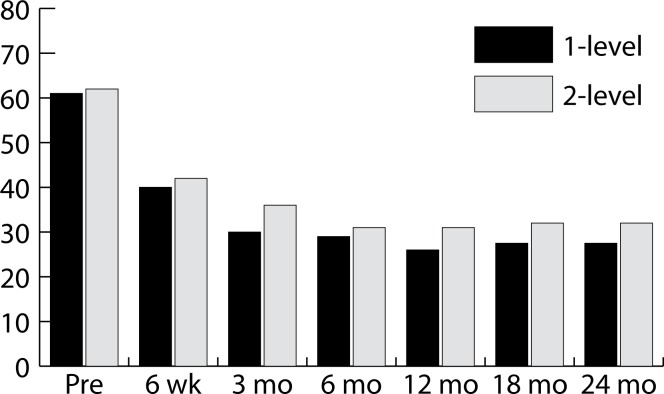
Results: Operative time and length of hospitalization were significantly less in the 1-level cases compared to 2 levels (61.6 min vs 97.8 min; and 1.89 days vs 2.44 days; P < .05). There was a trend for less blood loss in single-level cases (59.0 mL vs 79.2 mL) (.05 < P < .09). VAS and Oswestry scores were significantly improved in both groups postoperatively (by approximately 50%). At no follow-up were there significant differences in VAS, Oswestry, or patient satisfaction scores between the single- and 2-level patients. At all follow-ups, the mean satisfaction in both groups was greater than 7.5 on a scale of 0 to 10.
Conclusions: Patients undergoing 2-level TDR improved significantly postoperatively based on VAS and Oswestry scores, and there were no significant differences in outcome scores when comparing 1- and 2-level TDR.
Clinical relevance: This study suggests that 2-level TDR can be undertaken in appropriately selected patients and achieve results similar to singlelevel cases.
背景:融合术一直是治疗对非手术治疗无反应的疼痛性椎间盘退变的传统手术。在多节段手术中融合率可能下降。同时,融合也会对相邻椎间盘施加额外的压力。这种影响在多级程序中可能会被放大。单节段全椎间盘置换术(TDR)与融合术同样有效。关于两级TDR的已发表报告很少。本研究的目的是比较2级和1级手术的TDR结果。方法:本报告纳入了ProDisc-L试验性器械豁免(IDE)研究的首批连续86例患者,这些患者已达到24个月的随访,这些患者接受了1级(N = 54)或2级(N = 32)的TDR。临床结果测量包括评估疼痛的视觉模拟量表(VAS), Oswestry残疾指数,VAS测量的满意度,以及患者是否会再次进行相同手术的问题的回答。结果:1级患者的手术时间和住院时间明显少于2级患者(61.6 min vs 97.8 min;1.89天vs 2.44天;P < 0.05)。单水平病例的失血量有减少的趋势(59.0 mL vs 79.2 mL)。0.05 < p < .09)。两组术后VAS和Oswestry评分均显著提高(约50%)。在没有随访的情况下,单级和2级患者在VAS、Oswestry评分或患者满意度评分上没有显著差异。在所有的随访中,两组的平均满意度在0到10的范围内都大于7.5。结论:2级TDR患者术后VAS评分和Oswestry评分均有明显改善,1级TDR和2级TDR的结局评分比较无显著差异。临床相关性:本研究表明,2级TDR可以在适当选择的患者中进行,并获得与单级病例相似的结果。


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
