Liang Ke, Rebecca S Mason, Maina Kariuki, Elias Mpofu, Kaye E Brock
{"title":"Vitamin D status and hypertension: a review.","authors":"Liang Ke, Rebecca S Mason, Maina Kariuki, Elias Mpofu, Kaye E Brock","doi":"10.2147/IBPC.S49958","DOIUrl":null,"url":null,"abstract":"<p><p>Vitamin D is a steroid prohormone synthesized in the skin following ultraviolet exposure and also achieved through supplemental or dietary intake. While there is strong evidence for its role in maintaining bone and muscle health, there has been recent debate regarding the role of vitamin D deficiency in hypertension based on conflicting epidemiological evidence. Thus, we conducted a scoping systematic literature review and meta-analysis of all observational studies published up to early 2014 in order to map trends in the evidence of this association. Mixed-effect meta-analysis was performed to pool risk estimates from ten prospective studies (n=58,262) (pooled risk for incident hypertension, relative risk [RR] =0.76 (0.63-0.90) for top vs bottom category of 25-hydroxyvitamin D [25OHD]) and from 19 cross-sectional studies (n=90,535) (odds ratio [OR] =0.79 (0.73-0.87)). Findings suggest that the better the assessed quality of the respective study design, the stronger the relationship between higher 25OHD levels and hypertension risk (RR =0.67 (0.51-0.88); OR =0.77 (0.72-0.89)). There was significant heterogeneity among the findings for both prospective and cross-sectional studies, but no evidence of publication bias was shown. There was no increased risk of hypertension when the participants were of older age or when they were vitamin D deficient. Younger females showed strong associations between high 25OHD levels and hypertension risk, especially in prospective studies (RR =0.36 (0.18-0.72); OR =0.62 (0.44-0.87)). Despite the accumulating evidence of a consistent link between vitamin D and blood pressure, these data are observational, so questions still remain in relation to the causality of this relationship. Further studies either combining existing raw data from available cohort studies or conducting further Mendelian analyses are needed to determine whether this represents a causal association. Large randomized controlled trials are also needed to determine whether vitamin supplementation may be beneficial in the prevention or the treatment of hypertension. </p>","PeriodicalId":45299,"journal":{"name":"Integrated Blood Pressure Control","volume":"8 ","pages":"13-35"},"PeriodicalIF":2.7000,"publicationDate":"2015-04-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/IBPC.S49958","citationCount":"54","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated Blood Pressure Control","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IBPC.S49958","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 54
Abstract
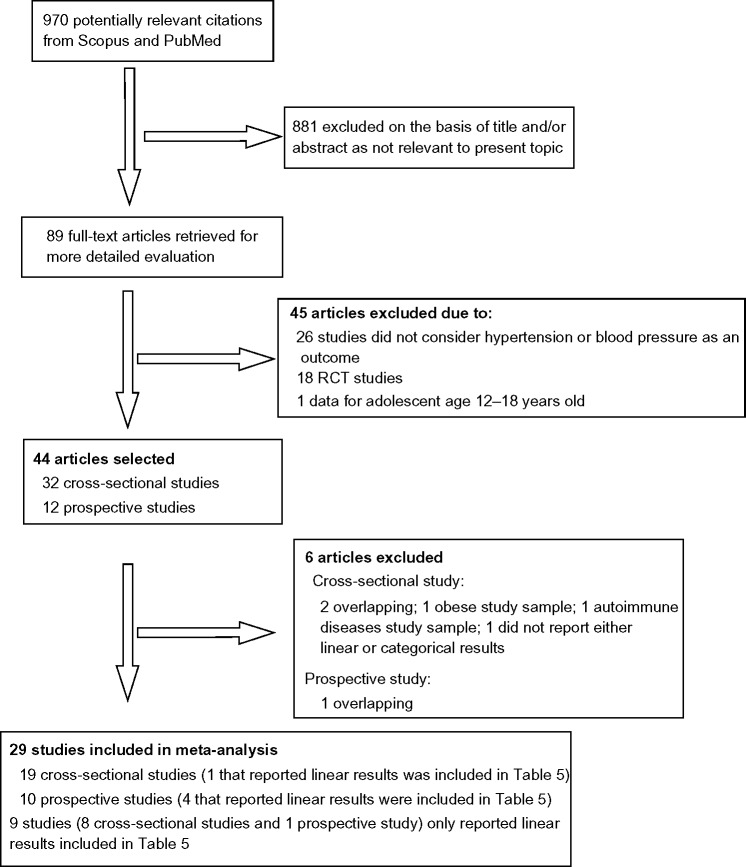
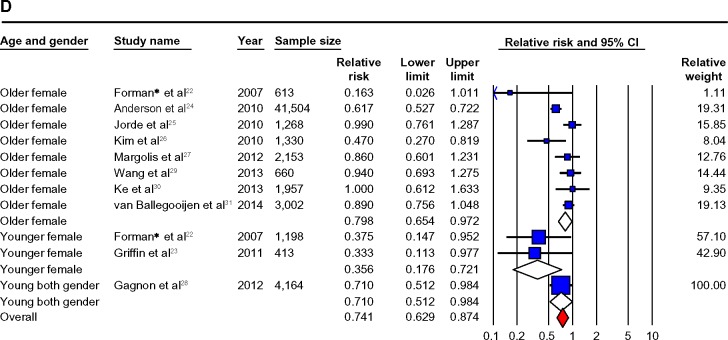
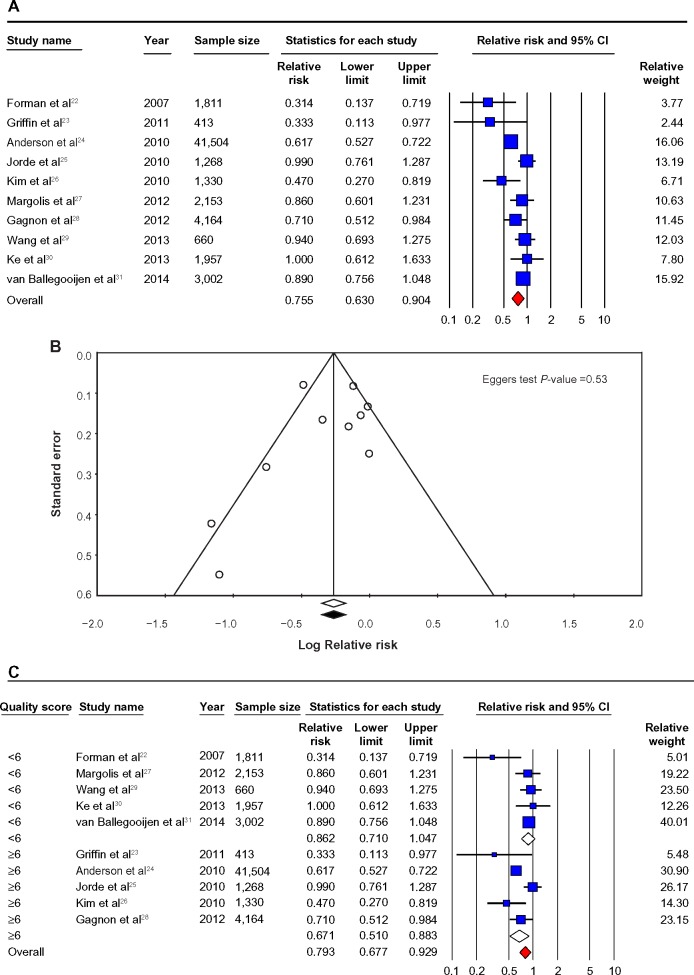
Vitamin D is a steroid prohormone synthesized in the skin following ultraviolet exposure and also achieved through supplemental or dietary intake. While there is strong evidence for its role in maintaining bone and muscle health, there has been recent debate regarding the role of vitamin D deficiency in hypertension based on conflicting epidemiological evidence. Thus, we conducted a scoping systematic literature review and meta-analysis of all observational studies published up to early 2014 in order to map trends in the evidence of this association. Mixed-effect meta-analysis was performed to pool risk estimates from ten prospective studies (n=58,262) (pooled risk for incident hypertension, relative risk [RR] =0.76 (0.63-0.90) for top vs bottom category of 25-hydroxyvitamin D [25OHD]) and from 19 cross-sectional studies (n=90,535) (odds ratio [OR] =0.79 (0.73-0.87)). Findings suggest that the better the assessed quality of the respective study design, the stronger the relationship between higher 25OHD levels and hypertension risk (RR =0.67 (0.51-0.88); OR =0.77 (0.72-0.89)). There was significant heterogeneity among the findings for both prospective and cross-sectional studies, but no evidence of publication bias was shown. There was no increased risk of hypertension when the participants were of older age or when they were vitamin D deficient. Younger females showed strong associations between high 25OHD levels and hypertension risk, especially in prospective studies (RR =0.36 (0.18-0.72); OR =0.62 (0.44-0.87)). Despite the accumulating evidence of a consistent link between vitamin D and blood pressure, these data are observational, so questions still remain in relation to the causality of this relationship. Further studies either combining existing raw data from available cohort studies or conducting further Mendelian analyses are needed to determine whether this represents a causal association. Large randomized controlled trials are also needed to determine whether vitamin supplementation may be beneficial in the prevention or the treatment of hypertension.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
