{"title":"The impact of the leg-lengthening total hip arthroplasty on the coronal alignment of the spine.","authors":"Yuichiro Abe, Shigenobu Sato, Satomi Abe, Takeshi Masuda, Kentaro Yamada","doi":"10.1186/1748-7161-10-S2-S4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Coronal imbalance of the pelvis is recognized to lead to the development of degenerative lumbar scoliosis. We hypothesized that an abrupt change of pelvic obliquity may show a reproducible trend of coronal compensation in the lumbosacral spine. The aim of the study was to classify the change of coronal alignment of spine after THA.</p><p><strong>Methods: </strong>This is a retrospective study based on the radiological analysis of 195 patients who underwent THA between 2009 and 2010. The mean age at surgery was 61.5 years old, and minimum follow up period was 24 months. Pelvic obliquity (POb) and Cobb's angle of lumbar scoliosis (LS) in coronal plane were measured. Over 3.5 degrees of change in POb was regarded as ΔPOb(+) and over 10 degrees of lumbar scoliosis was regarded as LS(+). The change of LS were classified into 3 subtypes; ΔLS(+), over 5 degrees of progress in LS, ΔLS(-), over 5 degrees of improvement in LS, and ΔLS(n), changes in LS within 5 degrees.</p><p><strong>Results: </strong>Over 3.5 degrees of change in POb was significantly correlated with the change in LS. Among195 patients, 120 patients improved their pelvic obliquity (ΔPOb(+)), and 75 patients did not have an improved pelvic obliquity (ΔPOb(-)). 99 patients out of 120 ΔPOb(+) patients did not show changes (54, ΔLS(n)) or improvement in scoliosis (45, ΔLS(-)).The remaining 21 patients showed progress or development of de novo scoliosis. Patients who failed to compensate for the POb change at lumbosacral area developed de novo lumbar scoliosis (7 cases), showed progression in lumbar scoliosis (7 cases) or developed coronal trunk shift over 20mm (7 cases).</p><p><strong>Conclusions: </strong>The patterns of compensation in lumbar or lumbosacral spine in coronal plane after leg lengthening THA were classified with regards to pelvic obliquity and Cobb's angle. 89.2% of 195 patients showed acceptable compensation in lumbar spine, 21 patients developed coronal imbalance. THA therefore is considered to be safe, as regards to spinal balance in coronal plane. However we have to keep in mind that preoperative rigid scoliosis could have a risk in progress for spinal imbalance.</p>","PeriodicalId":21722,"journal":{"name":"Scoliosis","volume":"10 Suppl 2","pages":"S4"},"PeriodicalIF":0.0000,"publicationDate":"2015-02-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/1748-7161-10-S2-S4","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scoliosis","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/1748-7161-10-S2-S4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 13
Abstract
Background: Coronal imbalance of the pelvis is recognized to lead to the development of degenerative lumbar scoliosis. We hypothesized that an abrupt change of pelvic obliquity may show a reproducible trend of coronal compensation in the lumbosacral spine. The aim of the study was to classify the change of coronal alignment of spine after THA.
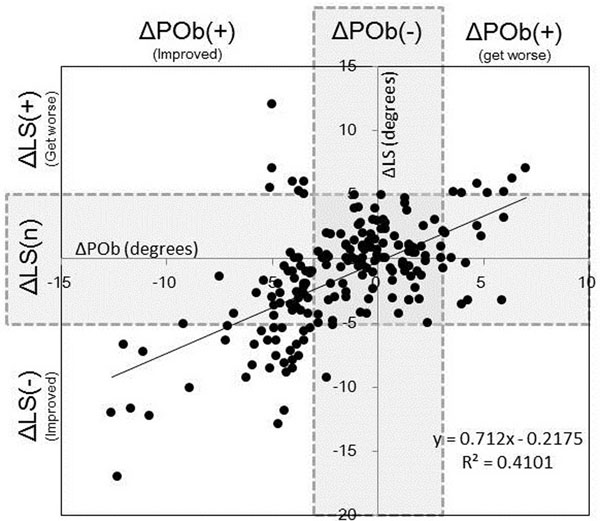
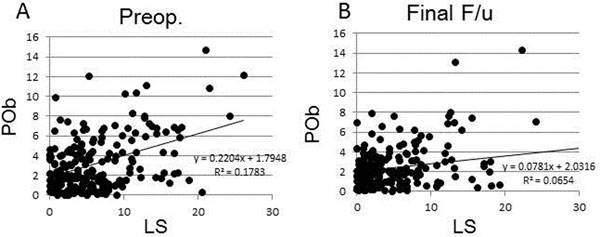
Methods: This is a retrospective study based on the radiological analysis of 195 patients who underwent THA between 2009 and 2010. The mean age at surgery was 61.5 years old, and minimum follow up period was 24 months. Pelvic obliquity (POb) and Cobb's angle of lumbar scoliosis (LS) in coronal plane were measured. Over 3.5 degrees of change in POb was regarded as ΔPOb(+) and over 10 degrees of lumbar scoliosis was regarded as LS(+). The change of LS were classified into 3 subtypes; ΔLS(+), over 5 degrees of progress in LS, ΔLS(-), over 5 degrees of improvement in LS, and ΔLS(n), changes in LS within 5 degrees.
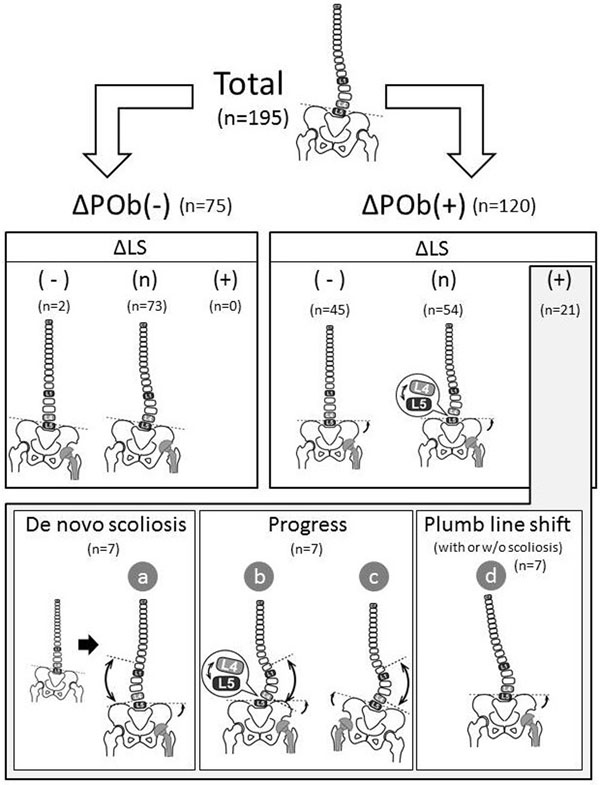
Results: Over 3.5 degrees of change in POb was significantly correlated with the change in LS. Among195 patients, 120 patients improved their pelvic obliquity (ΔPOb(+)), and 75 patients did not have an improved pelvic obliquity (ΔPOb(-)). 99 patients out of 120 ΔPOb(+) patients did not show changes (54, ΔLS(n)) or improvement in scoliosis (45, ΔLS(-)).The remaining 21 patients showed progress or development of de novo scoliosis. Patients who failed to compensate for the POb change at lumbosacral area developed de novo lumbar scoliosis (7 cases), showed progression in lumbar scoliosis (7 cases) or developed coronal trunk shift over 20mm (7 cases).
Conclusions: The patterns of compensation in lumbar or lumbosacral spine in coronal plane after leg lengthening THA were classified with regards to pelvic obliquity and Cobb's angle. 89.2% of 195 patients showed acceptable compensation in lumbar spine, 21 patients developed coronal imbalance. THA therefore is considered to be safe, as regards to spinal balance in coronal plane. However we have to keep in mind that preoperative rigid scoliosis could have a risk in progress for spinal imbalance.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
