G H Neild, Yuvaram N V Reddy, Yogesh N V Reddy, Deepika Lunawat, Georgi Abraham
{"title":"Successful management of angiomyolipoma of the left kidney.","authors":"G H Neild, Yuvaram N V Reddy, Yogesh N V Reddy, Deepika Lunawat, Georgi Abraham","doi":"10.1093/ndtplus/sfr101","DOIUrl":null,"url":null,"abstract":"A 57-year-old woman with a creatinine of 0.8 mg/dL and a normal urine analysis, was investigated with technetium-99m renogram and multidetector computerized tomography (MDCT) as a renal donor for her daughter. The glomerular filtration rate (GFR) was 100 mL/min with the left kidney 42 mL/min and right kidney 58 mL/ min. MDCT revealed a large lipomatous tumour on the renal cortex of the left lower pole with exophytic extension into the perirenal space measuring 7.3 3 5.2 cm (Figure 1). The arterial phase revealed dual arterial supply to the left kidney with the tumour being supplied by a branch from the lower renal artery (Figure 2a). The presence of fat [67 Hounsfield unit (HU)] with interposed soft tissue (42 HU), ectatic vessels and an aneurysm that measured 9 mm 3 8.9 mm with no direct arteriovenous shunting favoured the diagnosis of angiomyolipoma. Superselective catheterization of the feeding artery was performed and the neovascular vessels were embolized. Post-embolization MDCT revealed complete obliteration of the abnormal feeding artery and the aneurysmal lumen (Figure 2b). A week later, the GFR was 107 mL/min, left kidney 43 mL/min and right kidney 64 mL/min. Angiomyolipoma is a benign renal neoplasm with variable amounts of fat, vascular and smooth muscle elements. Attenuation of less than 20 HU on computerized tomography is widely accepted to confirm the presence of fat and this finding confirms the diagnosis of angiomyolipoma [1]. A tumour >4 cm with an aneurysm measuring >5 mm has a high risk of rupture [2].","PeriodicalId":18987,"journal":{"name":"NDT Plus","volume":"4 6","pages":"449-50"},"PeriodicalIF":0.0000,"publicationDate":"2011-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1093/ndtplus/sfr101","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"NDT Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ndtplus/sfr101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2011/8/24 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
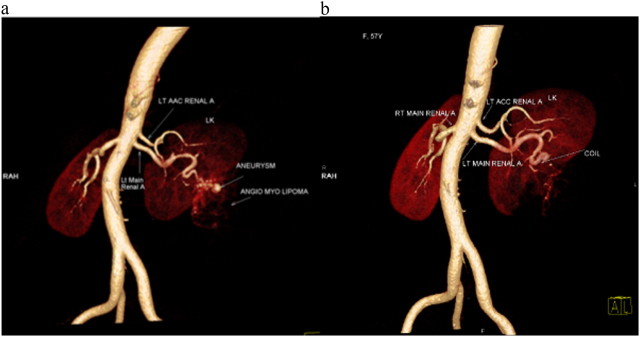
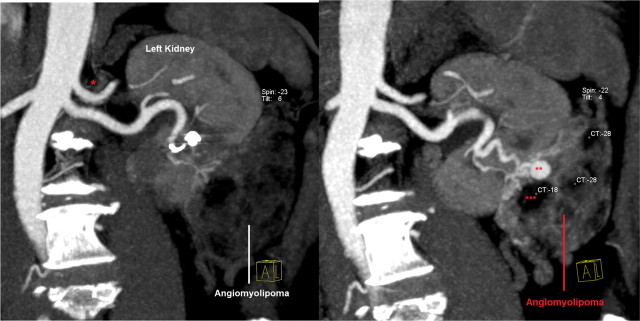
A 57-year-old woman with a creatinine of 0.8 mg/dL and a normal urine analysis, was investigated with technetium-99m renogram and multidetector computerized tomography (MDCT) as a renal donor for her daughter. The glomerular filtration rate (GFR) was 100 mL/min with the left kidney 42 mL/min and right kidney 58 mL/ min. MDCT revealed a large lipomatous tumour on the renal cortex of the left lower pole with exophytic extension into the perirenal space measuring 7.3 3 5.2 cm (Figure 1). The arterial phase revealed dual arterial supply to the left kidney with the tumour being supplied by a branch from the lower renal artery (Figure 2a). The presence of fat [67 Hounsfield unit (HU)] with interposed soft tissue (42 HU), ectatic vessels and an aneurysm that measured 9 mm 3 8.9 mm with no direct arteriovenous shunting favoured the diagnosis of angiomyolipoma. Superselective catheterization of the feeding artery was performed and the neovascular vessels were embolized. Post-embolization MDCT revealed complete obliteration of the abnormal feeding artery and the aneurysmal lumen (Figure 2b). A week later, the GFR was 107 mL/min, left kidney 43 mL/min and right kidney 64 mL/min. Angiomyolipoma is a benign renal neoplasm with variable amounts of fat, vascular and smooth muscle elements. Attenuation of less than 20 HU on computerized tomography is widely accepted to confirm the presence of fat and this finding confirms the diagnosis of angiomyolipoma [1]. A tumour >4 cm with an aneurysm measuring >5 mm has a high risk of rupture [2].


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
