Tighter or less tight glycaemic targets for women with gestational diabetes mellitus for reducing maternal and perinatal morbidity: A stepped-wedge, cluster-randomised trial.
Caroline A Crowther, Deborah Samuel, Ruth Hughes, Thach Tran, Julie Brown, Jane M Alsweiler
{"title":"Tighter or less tight glycaemic targets for women with gestational diabetes mellitus for reducing maternal and perinatal morbidity: A stepped-wedge, cluster-randomised trial.","authors":"Caroline A Crowther, Deborah Samuel, Ruth Hughes, Thach Tran, Julie Brown, Jane M Alsweiler","doi":"10.1371/journal.pmed.1004087","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Treatment for gestational diabetes mellitus (GDM) aims to reduce maternal hyperglycaemia. The TARGET Trial assessed whether tighter compared with less tight glycaemic control reduced maternal and perinatal morbidity.</p><p><strong>Methods and findings: </strong>In this stepped-wedge, cluster-randomised trial, identification number ACTRN12615000282583, 10 hospitals in New Zealand were randomised to 1 of 5 implementation dates. The trial was registered before the first participant was enrolled. All hospitals initially used less tight targets (fasting plasma glucose (FPG) <5.5 mmol/L (<99 mg/dL), 1-hour <8.0 mmol/L (<144 mg/dL), 2 hour postprandial <7.0 mmol/L (<126 mg/dL)) and every 4 months, 2 hospitals moved to use tighter targets (FPG ≤5.0 mmol/L (≤90 mg/dL), 1-hour ≤7.4 mmol/L (≤133 mg/dL), 2 hour postprandial ≤6.7 mmol/L) (≤121 mg/dL). Women with GDM, blinded to the targets in use, were eligible. The primary outcome was large for gestational age. Secondary outcomes assessed maternal and infant health. Analyses were by intention to treat. Between May 2015 and November 2017, data were collected from 1,100 women with GDM (1,108 infants); 598 women (602 infants) used the tighter targets and 502 women (506 infants) used the less tight targets. The rate of large for gestational age was similar between the treatment target groups (88/599, 14.7% versus 76/502, 15.1%; adjusted relative risk [adjRR] 0.96, 95% confidence interval [CI] 0.66 to 1.40, P = 0.839). The composite serious health outcome for the infant of perinatal death, birth trauma, or shoulder dystocia was apparently reduced in the tighter group when adjusted for gestational age at diagnosis of GDM, BMI, ethnicity, and history of GDM compared with the less tight group (8/599, 1.3% versus 13/505, 2.6%, adjRR 0.23, 95% CI 0.06 to 0.88, P = 0.032). No differences were seen for the other infant secondary outcomes apart from a shorter stay in intensive care (P = 0.041). Secondary outcomes for the woman showed an apparent increase for the composite serious health outcome that included major haemorrhage, coagulopathy, embolism, and obstetric complications in the tighter group (35/595, 5.9% versus 15/501, 3.0%, adjRR 2.29, 95% CI 1.14 to 4.59, P = 0.020). There were no differences between the target groups in the risk for pre-eclampsia, induction of labour, or cesarean birth, but more women using tighter targets required pharmacological treatment (404/595, 67.9% versus 293/501, 58.5%, adjRR 1.20, 95% CI 1.00 to 1.44, P = 0.047). The main study limitation is that the treatment targets used may vary to those in use in some countries.</p><p><strong>Conclusions: </strong>Tighter glycaemic targets in women with GDM compared to less tight targets did not reduce the risk of a large for gestational age infant, but did reduce serious infant morbidity, although serious maternal morbidity was increased. These findings can be used to aid decisions on the glycaemic targets women with GDM should use.</p><p><strong>Trial registration: </strong>The Australian New Zealand Clinical Trials Registry (ANZCTR). ACTRN12615000282583.</p>","PeriodicalId":20368,"journal":{"name":"PLoS Medicine","volume":"19 9","pages":"e1004087"},"PeriodicalIF":9.9000,"publicationDate":"2022-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9455881/pdf/","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLoS Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1371/journal.pmed.1004087","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 7
Abstract
Background: Treatment for gestational diabetes mellitus (GDM) aims to reduce maternal hyperglycaemia. The TARGET Trial assessed whether tighter compared with less tight glycaemic control reduced maternal and perinatal morbidity.
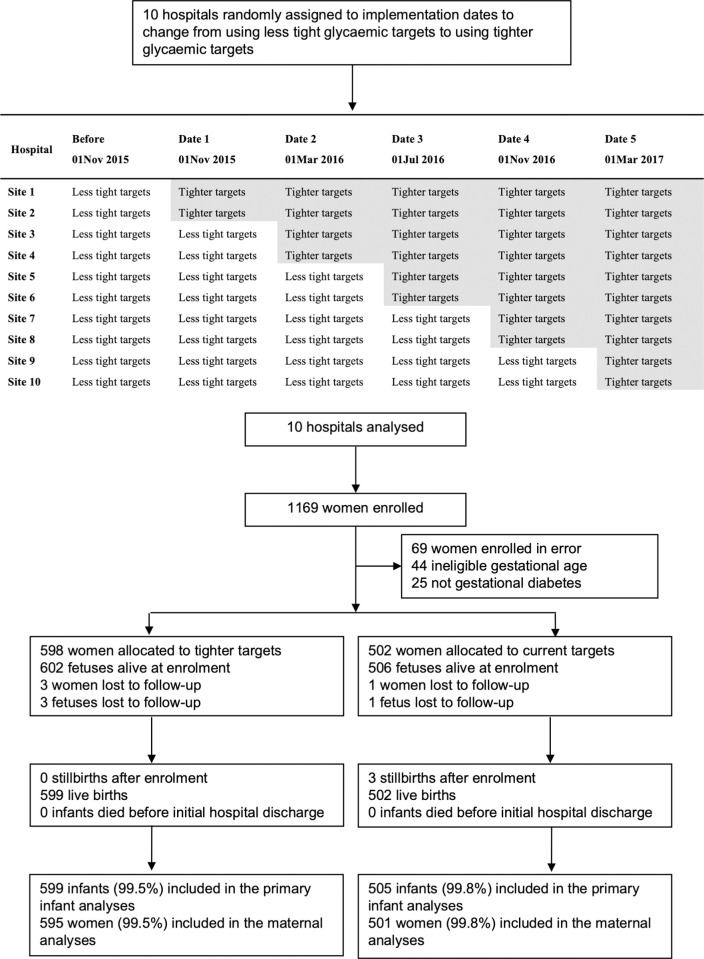
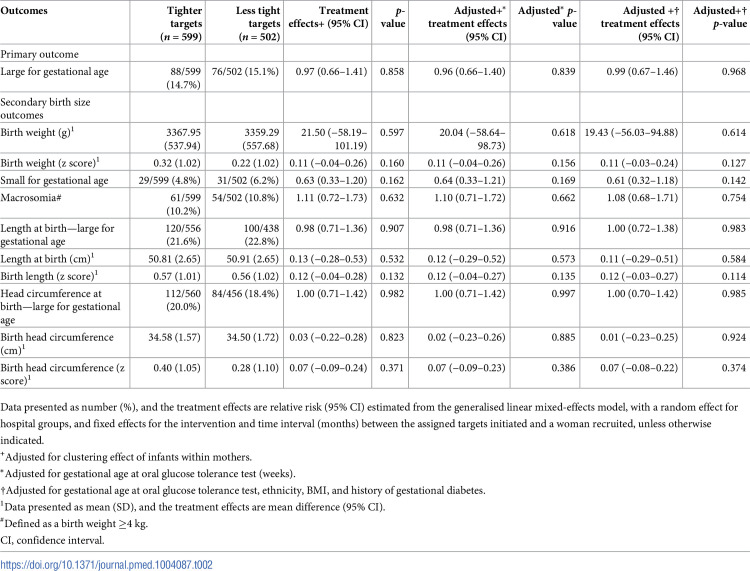
Methods and findings: In this stepped-wedge, cluster-randomised trial, identification number ACTRN12615000282583, 10 hospitals in New Zealand were randomised to 1 of 5 implementation dates. The trial was registered before the first participant was enrolled. All hospitals initially used less tight targets (fasting plasma glucose (FPG) <5.5 mmol/L (<99 mg/dL), 1-hour <8.0 mmol/L (<144 mg/dL), 2 hour postprandial <7.0 mmol/L (<126 mg/dL)) and every 4 months, 2 hospitals moved to use tighter targets (FPG ≤5.0 mmol/L (≤90 mg/dL), 1-hour ≤7.4 mmol/L (≤133 mg/dL), 2 hour postprandial ≤6.7 mmol/L) (≤121 mg/dL). Women with GDM, blinded to the targets in use, were eligible. The primary outcome was large for gestational age. Secondary outcomes assessed maternal and infant health. Analyses were by intention to treat. Between May 2015 and November 2017, data were collected from 1,100 women with GDM (1,108 infants); 598 women (602 infants) used the tighter targets and 502 women (506 infants) used the less tight targets. The rate of large for gestational age was similar between the treatment target groups (88/599, 14.7% versus 76/502, 15.1%; adjusted relative risk [adjRR] 0.96, 95% confidence interval [CI] 0.66 to 1.40, P = 0.839). The composite serious health outcome for the infant of perinatal death, birth trauma, or shoulder dystocia was apparently reduced in the tighter group when adjusted for gestational age at diagnosis of GDM, BMI, ethnicity, and history of GDM compared with the less tight group (8/599, 1.3% versus 13/505, 2.6%, adjRR 0.23, 95% CI 0.06 to 0.88, P = 0.032). No differences were seen for the other infant secondary outcomes apart from a shorter stay in intensive care (P = 0.041). Secondary outcomes for the woman showed an apparent increase for the composite serious health outcome that included major haemorrhage, coagulopathy, embolism, and obstetric complications in the tighter group (35/595, 5.9% versus 15/501, 3.0%, adjRR 2.29, 95% CI 1.14 to 4.59, P = 0.020). There were no differences between the target groups in the risk for pre-eclampsia, induction of labour, or cesarean birth, but more women using tighter targets required pharmacological treatment (404/595, 67.9% versus 293/501, 58.5%, adjRR 1.20, 95% CI 1.00 to 1.44, P = 0.047). The main study limitation is that the treatment targets used may vary to those in use in some countries.
Conclusions: Tighter glycaemic targets in women with GDM compared to less tight targets did not reduce the risk of a large for gestational age infant, but did reduce serious infant morbidity, although serious maternal morbidity was increased. These findings can be used to aid decisions on the glycaemic targets women with GDM should use.
Trial registration: The Australian New Zealand Clinical Trials Registry (ANZCTR). ACTRN12615000282583.
期刊介绍:
PLOS Medicine aims to be a leading platform for research and analysis on the global health challenges faced by humanity. The journal covers a wide range of topics, including biomedicine, the environment, society, and politics, that affect the well-being of individuals worldwide. It particularly highlights studies that contribute to clinical practice, health policy, or our understanding of disease mechanisms, with the ultimate goal of improving health outcomes in diverse settings.
Unwavering in its commitment to ethical standards, PLOS Medicine ensures integrity in medical publishing. This includes actively managing and transparently disclosing any conflicts of interest during the reporting, peer review, and publication processes. The journal promotes transparency by providing visibility into the review and publication procedures. It also encourages data sharing and the reuse of published work. Author rights are upheld, allowing them to retain copyright. Furthermore, PLOS Medicine strongly supports Open Access publishing, making research articles freely available to all without restrictions, facilitating widespread dissemination of knowledge. The journal does not endorse drug or medical device advertising and refrains from exclusive sales of reprints to avoid conflicts of interest.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
