Maria Grazia Pappalardo, Alessandra Di Nora, Andrea Giugno, Concetta Meli, Annamaria Sapuppo, Piero Pavone, Agata Fiumara
{"title":"Dihydropyridine Reductase Deficiency: Acute Encephalopathy Related to Folinic Acid Treatment Interruption in a Girl.","authors":"Maria Grazia Pappalardo, Alessandra Di Nora, Andrea Giugno, Concetta Meli, Annamaria Sapuppo, Piero Pavone, Agata Fiumara","doi":"10.1055/s-0042-1756661","DOIUrl":null,"url":null,"abstract":"<p><p>We reported the case of acute encephalopathy related to colonic acid treatment interruption in a 12-year-old female child presenting to our unit with episodes of vomiting, headache, irritability, acute confusional state, seizures, and left lower limb hypotonia. Brain magnetic resonance imaging (MRI) showed signs of vasogenic and cytotoxic edema at the cerebellar level bilaterally, and lesions at the temporo-occipito-parietal right level, temporomandibular left, and right thalamic with swelling of the convolutions and reduced differentiation between white and gray matter. The patient had suspended the folinic acid treatment at least 6 months before the present admission. The relation between the clinical signs presented by the girl and folic acid deficiency was confirmed by the result of laboratory assessment and by the answer to the notable clinical improvement with the renewal of folinic acid treatment. Dihydropteridine reductase (DHPR) deficiency is a rare autosomal recessive genetic disorder caused by the quinoid dihydropteridine reductase (QDPR) gene mutations. DHPR deficiency impairs the synthesis of the tetrahydrobiopterin (BH4), an essential cofactor for the hydroxylation of the aromatic amino acids phenylalanine, tyrosine, and tryptophan. When not precociously treated, the disorder may present whit severe neurologic impairment including developmental delay/intellective disability (DD/ID), microcephaly, seizures, movement disorders, cerebral palsy, and other neurological impairments. The clinical and neuroradiologic anomalies observed in our case were unusual, with signs previously unreported in patients with folic acid deficiency. The present case shows that the clinical presentation and MRI anomalies of the cerebral folic acid deficiency may be various and unusual compared with those reported in the literature, and it confirms the usefulness of the continuation of folinic acid treatment during the course of the disorder in patients with DHPR deficiency.</p>","PeriodicalId":40142,"journal":{"name":"Global Medical Genetics","volume":"9 3","pages":"247-251"},"PeriodicalIF":1.5000,"publicationDate":"2022-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9484871/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Medical Genetics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0042-1756661","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"GENETICS & HEREDITY","Score":null,"Total":0}
引用次数: 0
Abstract
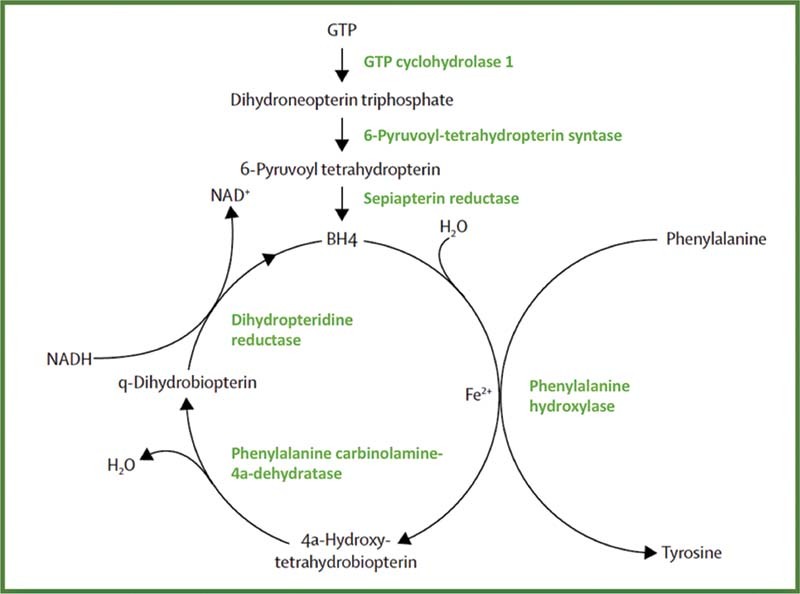
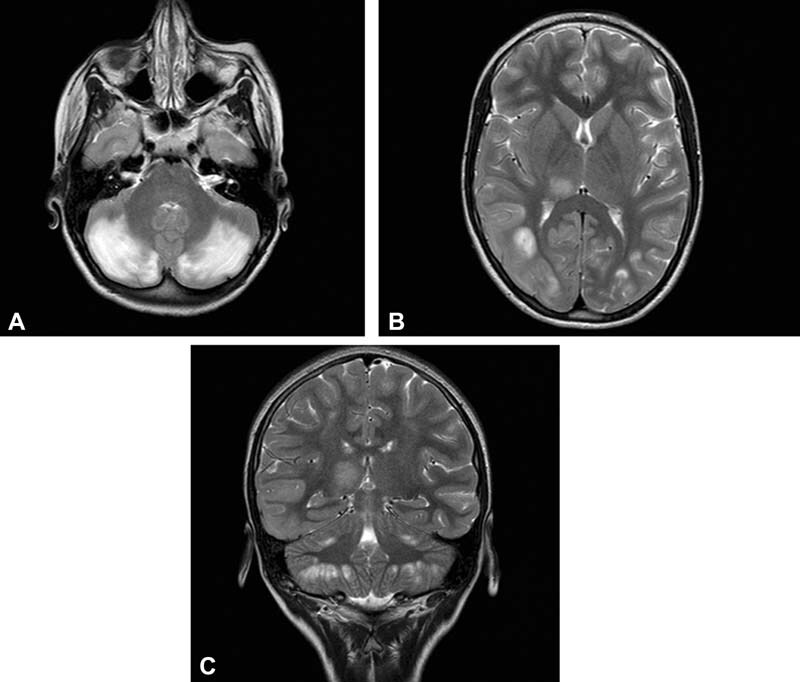
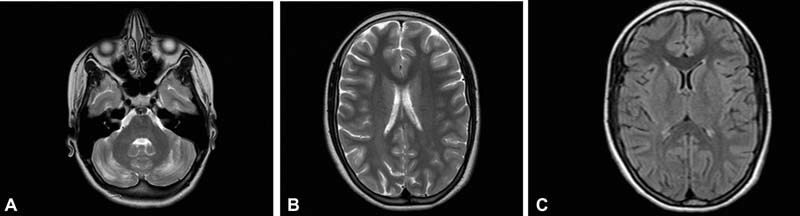
We reported the case of acute encephalopathy related to colonic acid treatment interruption in a 12-year-old female child presenting to our unit with episodes of vomiting, headache, irritability, acute confusional state, seizures, and left lower limb hypotonia. Brain magnetic resonance imaging (MRI) showed signs of vasogenic and cytotoxic edema at the cerebellar level bilaterally, and lesions at the temporo-occipito-parietal right level, temporomandibular left, and right thalamic with swelling of the convolutions and reduced differentiation between white and gray matter. The patient had suspended the folinic acid treatment at least 6 months before the present admission. The relation between the clinical signs presented by the girl and folic acid deficiency was confirmed by the result of laboratory assessment and by the answer to the notable clinical improvement with the renewal of folinic acid treatment. Dihydropteridine reductase (DHPR) deficiency is a rare autosomal recessive genetic disorder caused by the quinoid dihydropteridine reductase (QDPR) gene mutations. DHPR deficiency impairs the synthesis of the tetrahydrobiopterin (BH4), an essential cofactor for the hydroxylation of the aromatic amino acids phenylalanine, tyrosine, and tryptophan. When not precociously treated, the disorder may present whit severe neurologic impairment including developmental delay/intellective disability (DD/ID), microcephaly, seizures, movement disorders, cerebral palsy, and other neurological impairments. The clinical and neuroradiologic anomalies observed in our case were unusual, with signs previously unreported in patients with folic acid deficiency. The present case shows that the clinical presentation and MRI anomalies of the cerebral folic acid deficiency may be various and unusual compared with those reported in the literature, and it confirms the usefulness of the continuation of folinic acid treatment during the course of the disorder in patients with DHPR deficiency.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
