Geovedy Martinez-Garcia, Miguel Rodriguez-Ramos, Maikel Santos-Medina, Annia Maria Carrero-Vazquez, Yanitsy Chipi-Rodriguez
{"title":"New model predicts in-hospital complications in myocardial infarction.","authors":"Geovedy Martinez-Garcia, Miguel Rodriguez-Ramos, Maikel Santos-Medina, Annia Maria Carrero-Vazquez, Yanitsy Chipi-Rodriguez","doi":"10.15190/d.2022.1","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction and objectives: </strong>Ischemic cardiopathy constitutes the leading cause of death worldwide. Our aim was to evaluate the prognostic capacity of the leukoglycemic index as well as to create a predictive model of in-hospital complications in patients with ST elevation myocardial infarction.</p><p><strong>Materials and methods: </strong>This was a multicentral and cohort study, which included patients inserted in the Cuban Registry of acute myocardial infarction. The study investigated 900 patients with a validation population represented by 233 external subjects. In order to define the performance of the leukoglycemic index were evaluated the discrimination with the statistical C and the calibration by Hosmer - Lemeshow test. A model of logistic binary regression was employed in order to define the predictive factors. RESULTS: Optimal cut point of the leukoglycemic index to predict in-hospital complications was 1188 (sensibility 60%; specificity 61.6%; area under the curve 0.623; p < 0.001). In-hospital complications were significantly higher in the group with the leukoglycemic index ≥ 1188; a higher value was significantly associated with a higher risk to develop an in-hospital complication [RR (IC 95%) = 2.4 (1.804-3.080); p<0.001]. The predictive model proposed is composed by the following factors: age ≥ 66 years, leukoglycemic index ≥ 1188, Killip-Kimball classification ≥ II and medical history of hypertension. This scale had a good discrimination in both, the training and the validation population.</p><p><strong>Conclusion: </strong>The leukoglycemic index possesses a low performance when used to assess the risks for in hospital complications in patients with ST elevation myocardial infarction. The new predictive model has a good performance, which can be applied to estimate risk of in-hospital complications. This model would be able to contribute to the health systems of developing countries without additional cost; it enables prediction of the patients having a higher risk of complications and a negative outcome during the hospitable admission.</p>","PeriodicalId":72829,"journal":{"name":"Discoveries (Craiova, Romania)","volume":" ","pages":"e142"},"PeriodicalIF":0.0000,"publicationDate":"2022-03-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9482690/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Discoveries (Craiova, Romania)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.15190/d.2022.1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Introduction and objectives: Ischemic cardiopathy constitutes the leading cause of death worldwide. Our aim was to evaluate the prognostic capacity of the leukoglycemic index as well as to create a predictive model of in-hospital complications in patients with ST elevation myocardial infarction.
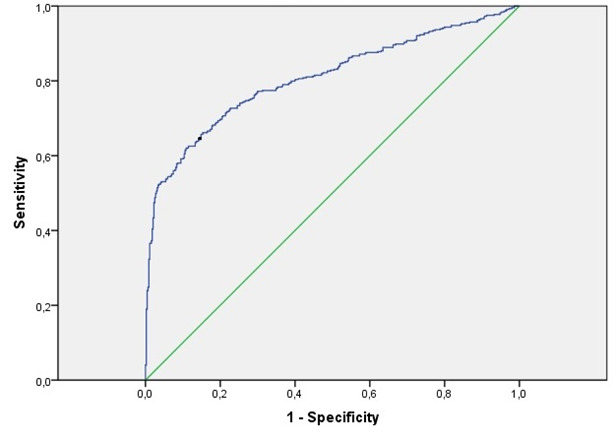
Materials and methods: This was a multicentral and cohort study, which included patients inserted in the Cuban Registry of acute myocardial infarction. The study investigated 900 patients with a validation population represented by 233 external subjects. In order to define the performance of the leukoglycemic index were evaluated the discrimination with the statistical C and the calibration by Hosmer - Lemeshow test. A model of logistic binary regression was employed in order to define the predictive factors. RESULTS: Optimal cut point of the leukoglycemic index to predict in-hospital complications was 1188 (sensibility 60%; specificity 61.6%; area under the curve 0.623; p < 0.001). In-hospital complications were significantly higher in the group with the leukoglycemic index ≥ 1188; a higher value was significantly associated with a higher risk to develop an in-hospital complication [RR (IC 95%) = 2.4 (1.804-3.080); p<0.001]. The predictive model proposed is composed by the following factors: age ≥ 66 years, leukoglycemic index ≥ 1188, Killip-Kimball classification ≥ II and medical history of hypertension. This scale had a good discrimination in both, the training and the validation population.
Conclusion: The leukoglycemic index possesses a low performance when used to assess the risks for in hospital complications in patients with ST elevation myocardial infarction. The new predictive model has a good performance, which can be applied to estimate risk of in-hospital complications. This model would be able to contribute to the health systems of developing countries without additional cost; it enables prediction of the patients having a higher risk of complications and a negative outcome during the hospitable admission.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
