Aortic remodelling and late outcomes following thoracic endovascular repair with a bare-metal stent distal extension among patients with complicated type-B aortic dissection.
Isaac Wamala, Mir Timo Zadegh Nazari-Shafti, Roland Heck, Adam Penkalla, Matteo Montagner, Steven J Staffa, Volkmar Falk, Semih Buz
{"title":"Aortic remodelling and late outcomes following thoracic endovascular repair with a bare-metal stent distal extension among patients with complicated type-B aortic dissection.","authors":"Isaac Wamala, Mir Timo Zadegh Nazari-Shafti, Roland Heck, Adam Penkalla, Matteo Montagner, Steven J Staffa, Volkmar Falk, Semih Buz","doi":"10.1093/icvts/ivac244","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>The goal of this study was to describe the factors affecting mid and late aortic remodelling following thoracic endovascular aortic repair with the PETTICOAT (Provisional Extension To Induce Complete Attachment) technique among patients with complicated acute or subacute type B aortic dissection.</p><p><strong>Methods: </strong>A retrospective single-centre study that evaluates clinical and morphological outcomes among 65 consecutive patients. The area and diameter of the true and false lumen, overall aortic diameter and false lumen perfusion were evaluated.</p><p><strong>Results: </strong>Concomitant direct visceral artery stenting was successfully conducted in 32 (49%) patients. There was one (1.5%) postoperative stroke; three (4.6%) patients developed spinal cord ischaemia; two (3%) patients suffered retrograde type A dissection; and two (3%) patients had mesenteric ischaemia, despite successful reperfusion, that required a bowel resection. Median postoperative follow-up was 63.1 (interquartile range, 32.1- 91.8) months. The probability of survival was 96.9% [95% confidence interval (CI) 88.3%-99.2%] at 30 days, 93.9% (95% CI 84.4%-97.6%) at 1 year, 78.0 (95% CI 64.2%-87.0%) at 5 years and 72.8% (95% CI at 57.9%-83.2%) at 10 years postoperatively. There was a statistically significant postoperative increase in true-lumen area, diameter and true-lumen index in all five aortic levels measured. Complete false lumen (FL) thrombosis at the coeliac trunk, renal arteries and aortic bifurcation levels was observed in 47%, 15% and 24% of patients at midterm (6-15 months) and in 29%, 21% and 29% on late (later than 21 months) computed tomography angiograms (CTA). Persistent false lumen (FL) perfusion at the coeliac level on midterm CTA was associated with a larger extent of late aortic growth (P = 0.042) and was, in the majority of cases, caused by iliac re-entries either alone (28.57) or in combination with visceral and lumbar (28.57%) or distal aortic (10.71%) re-entries. A larger abdominal aortic diameter at midterm was associated with an increased probability of distal aortic reinterventions (hazard ratio 7.26, 95% CI 2.41-21.9, P < 0.001).</p><p><strong>Conclusions: </strong>Persistent FL perfusion of the distal aorta at midterm following TEVAR with the PETTICOAT technique among patients with acute and subacute type B dissection is caused mainly by iliac, visceral, lumber and distal aorta re-entries. Patients with persistent FL perfusion have an increased risk of aortic aneurysmal growth at late follow-up.</p>","PeriodicalId":13621,"journal":{"name":"Interactive cardiovascular and thoracic surgery","volume":"35 5","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2022-10-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9553225/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interactive cardiovascular and thoracic surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/icvts/ivac244","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
Abstract
Objectives: The goal of this study was to describe the factors affecting mid and late aortic remodelling following thoracic endovascular aortic repair with the PETTICOAT (Provisional Extension To Induce Complete Attachment) technique among patients with complicated acute or subacute type B aortic dissection.
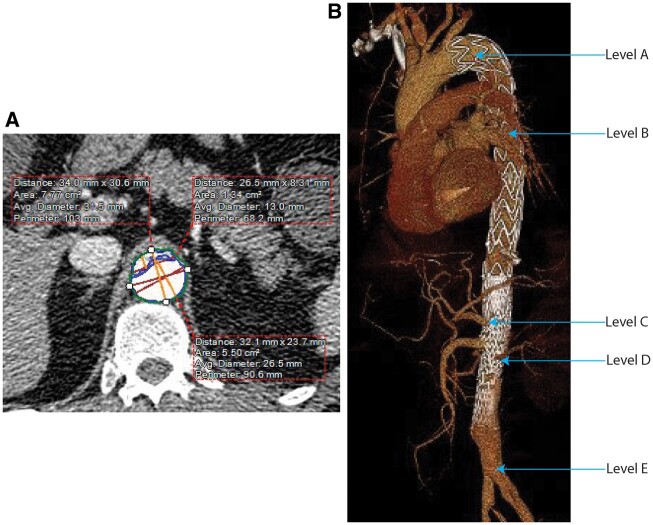
Methods: A retrospective single-centre study that evaluates clinical and morphological outcomes among 65 consecutive patients. The area and diameter of the true and false lumen, overall aortic diameter and false lumen perfusion were evaluated.
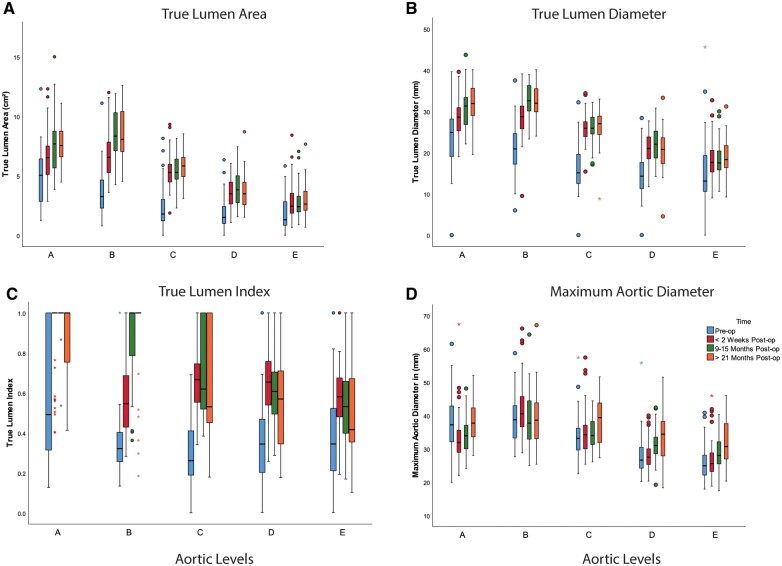
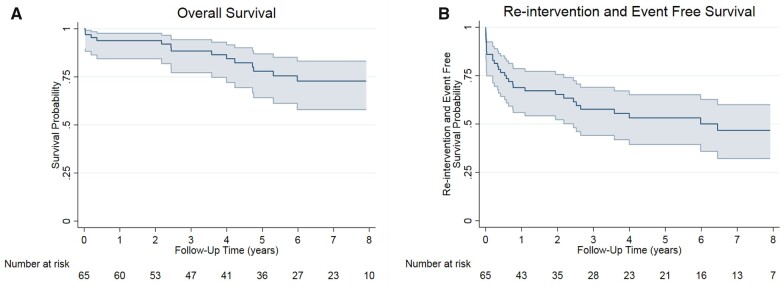
Results: Concomitant direct visceral artery stenting was successfully conducted in 32 (49%) patients. There was one (1.5%) postoperative stroke; three (4.6%) patients developed spinal cord ischaemia; two (3%) patients suffered retrograde type A dissection; and two (3%) patients had mesenteric ischaemia, despite successful reperfusion, that required a bowel resection. Median postoperative follow-up was 63.1 (interquartile range, 32.1- 91.8) months. The probability of survival was 96.9% [95% confidence interval (CI) 88.3%-99.2%] at 30 days, 93.9% (95% CI 84.4%-97.6%) at 1 year, 78.0 (95% CI 64.2%-87.0%) at 5 years and 72.8% (95% CI at 57.9%-83.2%) at 10 years postoperatively. There was a statistically significant postoperative increase in true-lumen area, diameter and true-lumen index in all five aortic levels measured. Complete false lumen (FL) thrombosis at the coeliac trunk, renal arteries and aortic bifurcation levels was observed in 47%, 15% and 24% of patients at midterm (6-15 months) and in 29%, 21% and 29% on late (later than 21 months) computed tomography angiograms (CTA). Persistent false lumen (FL) perfusion at the coeliac level on midterm CTA was associated with a larger extent of late aortic growth (P = 0.042) and was, in the majority of cases, caused by iliac re-entries either alone (28.57) or in combination with visceral and lumbar (28.57%) or distal aortic (10.71%) re-entries. A larger abdominal aortic diameter at midterm was associated with an increased probability of distal aortic reinterventions (hazard ratio 7.26, 95% CI 2.41-21.9, P < 0.001).
Conclusions: Persistent FL perfusion of the distal aorta at midterm following TEVAR with the PETTICOAT technique among patients with acute and subacute type B dissection is caused mainly by iliac, visceral, lumber and distal aorta re-entries. Patients with persistent FL perfusion have an increased risk of aortic aneurysmal growth at late follow-up.
期刊介绍:
Interactive CardioVascular and Thoracic Surgery (ICVTS) publishes scientific contributions in the field of cardiovascular and thoracic surgery, covering all aspects of surgery of the heart, vessels and the chest. The journal publishes a range of article types including: Best Evidence Topics; Brief Communications; Case Reports; Original Articles; State-of-the-Art; Work in Progress Report.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
