Abdulhadi Jfri, Bonnie Leung, Jordan T Said, Yevgeniy Semenov, Nicole R LeBoeuf
{"title":"Prevalence of inverse psoriasis subtype with immune checkpoint inhibitors.","authors":"Abdulhadi Jfri, Bonnie Leung, Jordan T Said, Yevgeniy Semenov, Nicole R LeBoeuf","doi":"10.1093/immadv/ltac016","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cutaneous immune-related adverse events (irAEs) are the most common irAEs caused by immune-checkpoint inhibitors (ICI). Psoriasiform eruptions, both <i>de novo</i> and flares, may occur. Evidence is lacking on inverse psoriasis subtype.</p><p><strong>Methods: </strong>A retrospective study was conducted at Dana-Farber Cancer Institute/Mass General Brigham through February 2020 using databases. Confirmed inverse psoriasis cases pre-/post-ICI initiation either independently or in conjunction with other psoriasis subtypes were included. Known psoriasis cases without flare post-ICI were excluded.</p><p><strong>Results: </strong>A total of 262 (3%) individuals with any ICI-mediated psoriasiform cutaneous irAE were identified out of the 8683 DFCI ICI-treated patients. Of these, 13 (5% of psoriasis patients) had inverse psoriasis (mean age 68.7 years; 7/13 male sex). Median (range) time from ICI initiation to inverse psoriasis development or flare was 7 (4-12) and 3.5 (2-6) weeks, respectively. Pruritus occurred in 12/13 (92.30%) cases. 11 (85%) had inguinal involvement; other sites included gluteal cleft (6; 46%), inframammary (3; 23%), perianal (2; 15%), axilla (2; 15%), umbilicus (2; 15%), and infra-abdominal folds (1; 8%). Most (9/13) individuals had more than one site involved. The Common Terminology Criteria for Adverse Events severity was 1 in 10 (76.92%) individuals and 2 in 3 (15.38%) individuals. Six (46.15%) patients were treated initially by oncology with topical (nystatin, econazole, or clotrimazole) or systemic antifungals (fluconazole) for median (range) of 3.5 (1-7) months without improvement, for presumed candida intertrigo.</p><p><strong>Conclusion: </strong>Patients on ICI may develop inverse psoriasis, which may be initially confused for fungal intertrigo. Delayed diagnosis can prolong symptoms, while patients are treated ineffectively with topical/systemic antifungals for presumed candida infection. Oncologist and dermatologist awareness is important to improve diagnosis of ICI-mediated inverse psoriasis, its management and affected patients' quality of life.</p>","PeriodicalId":4,"journal":{"name":"ACS Applied Energy Materials","volume":" ","pages":"ltac016"},"PeriodicalIF":5.5000,"publicationDate":"2022-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/60/68/ltac016.PMC9525015.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ACS Applied Energy Materials","FirstCategoryId":"88","ListUrlMain":"https://doi.org/10.1093/immadv/ltac016","RegionNum":3,"RegionCategory":"材料科学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CHEMISTRY, PHYSICAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Cutaneous immune-related adverse events (irAEs) are the most common irAEs caused by immune-checkpoint inhibitors (ICI). Psoriasiform eruptions, both de novo and flares, may occur. Evidence is lacking on inverse psoriasis subtype.
Methods: A retrospective study was conducted at Dana-Farber Cancer Institute/Mass General Brigham through February 2020 using databases. Confirmed inverse psoriasis cases pre-/post-ICI initiation either independently or in conjunction with other psoriasis subtypes were included. Known psoriasis cases without flare post-ICI were excluded.
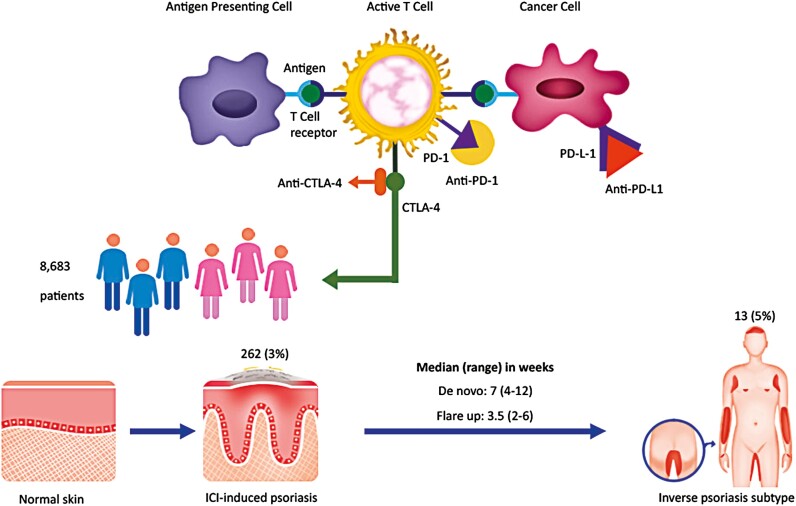
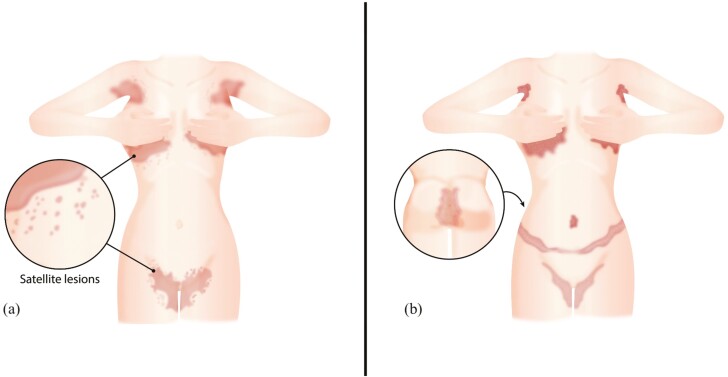
Results: A total of 262 (3%) individuals with any ICI-mediated psoriasiform cutaneous irAE were identified out of the 8683 DFCI ICI-treated patients. Of these, 13 (5% of psoriasis patients) had inverse psoriasis (mean age 68.7 years; 7/13 male sex). Median (range) time from ICI initiation to inverse psoriasis development or flare was 7 (4-12) and 3.5 (2-6) weeks, respectively. Pruritus occurred in 12/13 (92.30%) cases. 11 (85%) had inguinal involvement; other sites included gluteal cleft (6; 46%), inframammary (3; 23%), perianal (2; 15%), axilla (2; 15%), umbilicus (2; 15%), and infra-abdominal folds (1; 8%). Most (9/13) individuals had more than one site involved. The Common Terminology Criteria for Adverse Events severity was 1 in 10 (76.92%) individuals and 2 in 3 (15.38%) individuals. Six (46.15%) patients were treated initially by oncology with topical (nystatin, econazole, or clotrimazole) or systemic antifungals (fluconazole) for median (range) of 3.5 (1-7) months without improvement, for presumed candida intertrigo.
Conclusion: Patients on ICI may develop inverse psoriasis, which may be initially confused for fungal intertrigo. Delayed diagnosis can prolong symptoms, while patients are treated ineffectively with topical/systemic antifungals for presumed candida infection. Oncologist and dermatologist awareness is important to improve diagnosis of ICI-mediated inverse psoriasis, its management and affected patients' quality of life.
期刊介绍:
ACS Applied Energy Materials is an interdisciplinary journal publishing original research covering all aspects of materials, engineering, chemistry, physics and biology relevant to energy conversion and storage. The journal is devoted to reports of new and original experimental and theoretical research of an applied nature that integrate knowledge in the areas of materials, engineering, physics, bioscience, and chemistry into important energy applications.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
