Complete transurethral resection of bladder tumor before radical cystectomy is not a risk factor for organ-confined bladder cancer: A case-control study.
{"title":"Complete transurethral resection of bladder tumor before radical cystectomy is not a risk factor for organ-confined bladder cancer: A case-control study.","authors":"Xiaoxu Yuan, Mingkun Chen, Jing Yang, Yunlin Ye","doi":"10.1097/CU9.0000000000000110","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To investigate the role of complete transurethral resection of bladder tumor (TURBT) before radical cystectomy (RC) for organ-confined bladder cancer.</p><p><strong>Materials and methods: </strong>Data of patients who underwent RC in our center from January 2008 to December 2018 were retrospectively reviewed. Patients with >T2N0M0 disease and positive surgical margins and those who received neoadjuvant/adjuvant chemotherapy or radiotherapy were excluded. Complete TURBT was defined as no visible lesion under endoscopic examination after TURBT or in the bladder specimen after RC. Kaplan-Meier curves and log-rank tests assessed disease-free survival (DFS). Logistic and Cox regression analyses were performed to identify potential predictors.</p><p><strong>Results: </strong>A total of 236 patients were included in this review, including 207 males, with a median age of 61 years. The median tumor size was 3 cm, and a total of 94 patients had identified pathological T2 stage disease. Complete TURBT was correlated with tumor size (<i>p</i> = 0.041), histological variants (<i>p</i> = 0.026), and down-staging (<i>p</i> < 0.001). Tumor size, grade, and histological variants were independent predictors of complete TURBT. During a median follow-up of 42.7 months, 30 patients developed disease recurrence. Age and histological variants were independent predictors of DFS (<i>p</i> = 0.022 and 0.032, respectively), whereas complete TURBT was not an independent predictor of DFS (<i>p</i> = 0.156). Down-staging was not associated with survival outcome.</p><p><strong>Conclusions: </strong>Complete TURBT was correlated with an increased rate of down-staging before RC. It was not associated with better oncologic outcomes for patients with organ-confined bladder cancer.</p>","PeriodicalId":39147,"journal":{"name":"Current Urology","volume":"16 3","pages":"142-146"},"PeriodicalIF":1.3000,"publicationDate":"2022-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/2c/16/curr-urol-16-142.PMC9527917.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CU9.0000000000000110","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/8/27 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To investigate the role of complete transurethral resection of bladder tumor (TURBT) before radical cystectomy (RC) for organ-confined bladder cancer.
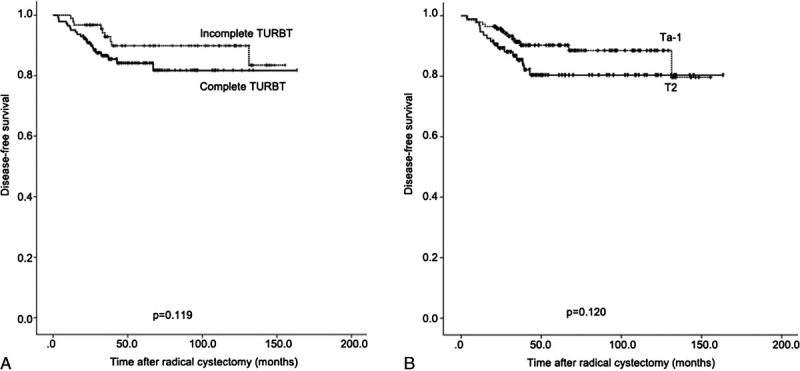
Materials and methods: Data of patients who underwent RC in our center from January 2008 to December 2018 were retrospectively reviewed. Patients with >T2N0M0 disease and positive surgical margins and those who received neoadjuvant/adjuvant chemotherapy or radiotherapy were excluded. Complete TURBT was defined as no visible lesion under endoscopic examination after TURBT or in the bladder specimen after RC. Kaplan-Meier curves and log-rank tests assessed disease-free survival (DFS). Logistic and Cox regression analyses were performed to identify potential predictors.
Results: A total of 236 patients were included in this review, including 207 males, with a median age of 61 years. The median tumor size was 3 cm, and a total of 94 patients had identified pathological T2 stage disease. Complete TURBT was correlated with tumor size (p = 0.041), histological variants (p = 0.026), and down-staging (p < 0.001). Tumor size, grade, and histological variants were independent predictors of complete TURBT. During a median follow-up of 42.7 months, 30 patients developed disease recurrence. Age and histological variants were independent predictors of DFS (p = 0.022 and 0.032, respectively), whereas complete TURBT was not an independent predictor of DFS (p = 0.156). Down-staging was not associated with survival outcome.
Conclusions: Complete TURBT was correlated with an increased rate of down-staging before RC. It was not associated with better oncologic outcomes for patients with organ-confined bladder cancer.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
