{"title":"Early versus Late Tracheostomy in Patients with Acute Brain Injury: Importance of SET Score.","authors":"Saurav Shekhar, Raj Bahadur Singh, Ranjeet Rana De, Ritu Singh, Akhileshwar, Nitin Kumar","doi":"10.4103/aer.aer_22_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Patients with acute brain injury presents are unique subset of neurocritical care patients with its long-term functional prognosis difficult to determine. They often have long intensive care unit (ICU) stay and presents as challenge to decide when to transfer out of ICU. This prospective study aims to assess the benefits of early tracheostomy in terms of ICU-length of stay (ICU-LOS), number of days on ventilator (ventilator days), incidence of ventilator-associated pneumonia (VAP), and mortality rates.</p><p><strong>Materials and methods: </strong>After institutional ethical clearance, 80 patients were randomized into two groups: Group A, early tracheostomy group (tracheostomy within 3 days of intubation) and Group B, standard of care group (tracheostomy after 10 days of intubation: late tracheostomy). A cutoff of 10 in the SET score was used in predicting need of early tracheostomy; both groups were compared with respect to ICU-LOS, number of ventilator days (ventilation time), need of analgesia and sedation, incidence of VAP, and mortality data.</p><p><strong>Results: </strong>Both the groups were comparable in terms of demographic profile and various disease severity scores. ICU-LOS was 14.9 ± 3.6 days in Group A and 17.2 ± 4.6 in Group B. The number of days on ventilator and incidence of VAP was significantly lower in Group A as compared to Group B. There was significantly lower mortality in Group A subset of patients in ICU.</p><p><strong>Conclusion: </strong>SET score is a simple and reliable score with fair accuracy and high sensitivity and specificity in predicting need of tracheostomy in neurocritical patients. A cutoff of 10 in the score can be reliably used in predicting need of early tracheostomy as in few other studies. Early tracheostomy is clearly advantageous in neurocritical patients, but has no advantage in terms of long-term mortality rates.</p>","PeriodicalId":7798,"journal":{"name":"Anesthesia, Essays and Researches","volume":"16 1","pages":"7-11"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9558650/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia, Essays and Researches","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/aer.aer_22_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/5/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Introduction: Patients with acute brain injury presents are unique subset of neurocritical care patients with its long-term functional prognosis difficult to determine. They often have long intensive care unit (ICU) stay and presents as challenge to decide when to transfer out of ICU. This prospective study aims to assess the benefits of early tracheostomy in terms of ICU-length of stay (ICU-LOS), number of days on ventilator (ventilator days), incidence of ventilator-associated pneumonia (VAP), and mortality rates.
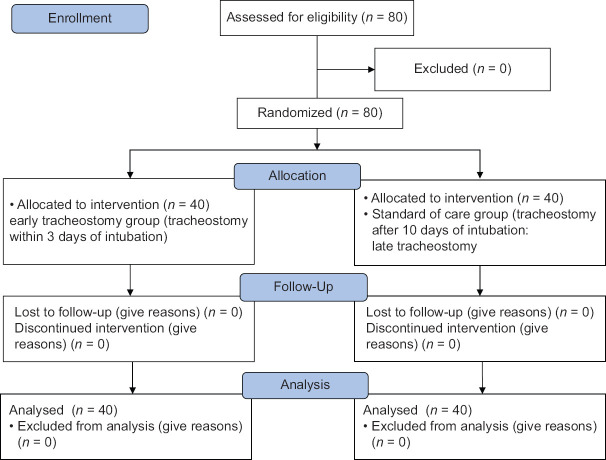
Materials and methods: After institutional ethical clearance, 80 patients were randomized into two groups: Group A, early tracheostomy group (tracheostomy within 3 days of intubation) and Group B, standard of care group (tracheostomy after 10 days of intubation: late tracheostomy). A cutoff of 10 in the SET score was used in predicting need of early tracheostomy; both groups were compared with respect to ICU-LOS, number of ventilator days (ventilation time), need of analgesia and sedation, incidence of VAP, and mortality data.
Results: Both the groups were comparable in terms of demographic profile and various disease severity scores. ICU-LOS was 14.9 ± 3.6 days in Group A and 17.2 ± 4.6 in Group B. The number of days on ventilator and incidence of VAP was significantly lower in Group A as compared to Group B. There was significantly lower mortality in Group A subset of patients in ICU.
Conclusion: SET score is a simple and reliable score with fair accuracy and high sensitivity and specificity in predicting need of tracheostomy in neurocritical patients. A cutoff of 10 in the score can be reliably used in predicting need of early tracheostomy as in few other studies. Early tracheostomy is clearly advantageous in neurocritical patients, but has no advantage in terms of long-term mortality rates.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
