David M Charytan, Angeles Cinelli, Elisabeth M Zeisberg
{"title":"Association of circulating angiogenesis inhibitors and asymmetric dimethyl arginine with coronary plaque burden.","authors":"David M Charytan, Angeles Cinelli, Elisabeth M Zeisberg","doi":"10.1186/s13069-015-0029-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Chronic kidney disease (CKD) is an independent risk factor for the development and severity of coronary artery disease (CHD) and endothelial dysfunction. There is an increase in the circulating angiogenesis inhibitors endostatin (END), thrombospondin-2 (TSP), angiopoietin-2 (ANG) and the nitric oxide (NO) inhibitor asymmetric dimethyl arginine (ADMA) in CKD patients. The aim of this study was to evaluate associations of the serum level of these factors and of the related angiogenesis inhibitor, endoglin (ENG), with burden of coronary atherosclerosis.</p><p><strong>Methods: </strong>One hundred twenty-two patients undergoing coronary angiography were recruited from the cardiac catheterization lab at a single center. The total burden of coronary plaque (mm(2)) and the presence of coronary collaterals were quantified using quantitative coronary angiography (QCA). Serum levels of angiogenesis inhibitors were measured by ELISA (ENG, END, and ANG), Luminex assay (TSP), or HLPC (ADMA), respectively. Associations with plaque burden and coronary collateral supply were analyzed in multi-variable linear and logistic regression models.</p><p><strong>Results: </strong>There was no significant association found between levels of circulating ADMA, ENG, END, ANG, or TSP and coronary plaque burden or collateral formation.</p><p><strong>Conclusions: </strong>Our findings suggest that associations of circulating END, ENG, TSP, and ANG with cardiovascular mortality are unlikely to be mediated via direct effects on coronary plaque formation or by inhibition of collateral formation. Whether associations of these factors with mortality are mediated via local concentrations, myocardial tissue, or intra-plaque expression of these factors or by an effect on plaque vulnerability merits additional investigation.</p>","PeriodicalId":12264,"journal":{"name":"Fibrogenesis & Tissue Repair","volume":"8 ","pages":"13"},"PeriodicalIF":0.0000,"publicationDate":"2015-07-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13069-015-0029-6","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Fibrogenesis & Tissue Repair","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13069-015-0029-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 11
Abstract
Background: Chronic kidney disease (CKD) is an independent risk factor for the development and severity of coronary artery disease (CHD) and endothelial dysfunction. There is an increase in the circulating angiogenesis inhibitors endostatin (END), thrombospondin-2 (TSP), angiopoietin-2 (ANG) and the nitric oxide (NO) inhibitor asymmetric dimethyl arginine (ADMA) in CKD patients. The aim of this study was to evaluate associations of the serum level of these factors and of the related angiogenesis inhibitor, endoglin (ENG), with burden of coronary atherosclerosis.
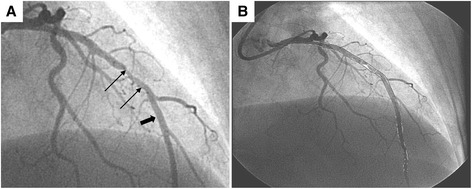
Methods: One hundred twenty-two patients undergoing coronary angiography were recruited from the cardiac catheterization lab at a single center. The total burden of coronary plaque (mm(2)) and the presence of coronary collaterals were quantified using quantitative coronary angiography (QCA). Serum levels of angiogenesis inhibitors were measured by ELISA (ENG, END, and ANG), Luminex assay (TSP), or HLPC (ADMA), respectively. Associations with plaque burden and coronary collateral supply were analyzed in multi-variable linear and logistic regression models.
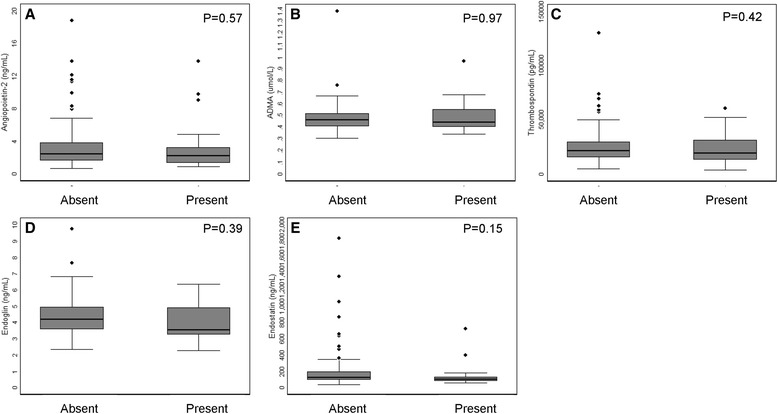
Results: There was no significant association found between levels of circulating ADMA, ENG, END, ANG, or TSP and coronary plaque burden or collateral formation.
Conclusions: Our findings suggest that associations of circulating END, ENG, TSP, and ANG with cardiovascular mortality are unlikely to be mediated via direct effects on coronary plaque formation or by inhibition of collateral formation. Whether associations of these factors with mortality are mediated via local concentrations, myocardial tissue, or intra-plaque expression of these factors or by an effect on plaque vulnerability merits additional investigation.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
