Jordan Chenkin, Colin J L McCartney, Tomislav Jelic, Michael Romano, Claire Heslop, Glen Bandiera
{"title":"Defining the learning curve of point-of-care ultrasound for confirming endotracheal tube placement by emergency physicians.","authors":"Jordan Chenkin, Colin J L McCartney, Tomislav Jelic, Michael Romano, Claire Heslop, Glen Bandiera","doi":"10.1186/s13089-015-0031-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Unrecognized esophageal intubations are associated with significant patient morbidity and mortality. No single confirmatory device has been shown to be 100 % accurate at ruling out esophageal intubations in the emergency department. Recent studies have demonstrated that point-of-care ultrasound (POCUS) may be a useful adjunct for confirming endotracheal tube placement; however, the amount of practice required to become proficient at this technique is unclear. The purpose of this study is to determine the amount of practice required by emergency physicians to become proficient at interpreting ultrasound video clips of esophageal and endotracheal intubations.</p><p><strong>Methods: </strong>Emergency physicians and emergency medicine residents completed a baseline interpretation test followed by a 10 min online tutorial. They then interpreted POCUS clips of esophageal and endotracheal intubations in a randomly selected order. If an incorrect response was provided, the participant completed another practice session with feedback. This process continued until they correctly interpreted ten consecutive ultrasound clips. Descriptive statistics were used to summarize the data.</p><p><strong>Results: </strong>Of the 87 eligible physicians, 66 (75.9 %) completed the study. The mean score on the baseline test was 42.9 % (SD 32.7 %). After the tutorial, 90.9 % (60/66) of the participants achieved proficiency after one practice attempt and 100 % achieved proficiency after two practice attempts. Six intubation ultrasound clips were misinterpreted, for a total error rate of 0.9 % (6/684). Overall, the participants had a sensitivity of 98.3 % (95 % CI 96.3-99.4 %) and specificity of 100 % (95 % CI 98.9-100 %) for detecting correct tube location. Scans were interpreted within an average of 4 s (SD 2.9 s) of the intubation.</p><p><strong>Conclusions: </strong>After a brief online tutorial and only two practice attempts, emergency physicians were able to quickly and accurately interpret ultrasound intubation clips of esophageal and endotracheal intubations.</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"7 1","pages":"14"},"PeriodicalIF":3.6000,"publicationDate":"2015-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-015-0031-7","citationCount":"47","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-015-0031-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/9/17 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 47
Abstract
Background: Unrecognized esophageal intubations are associated with significant patient morbidity and mortality. No single confirmatory device has been shown to be 100 % accurate at ruling out esophageal intubations in the emergency department. Recent studies have demonstrated that point-of-care ultrasound (POCUS) may be a useful adjunct for confirming endotracheal tube placement; however, the amount of practice required to become proficient at this technique is unclear. The purpose of this study is to determine the amount of practice required by emergency physicians to become proficient at interpreting ultrasound video clips of esophageal and endotracheal intubations.
Methods: Emergency physicians and emergency medicine residents completed a baseline interpretation test followed by a 10 min online tutorial. They then interpreted POCUS clips of esophageal and endotracheal intubations in a randomly selected order. If an incorrect response was provided, the participant completed another practice session with feedback. This process continued until they correctly interpreted ten consecutive ultrasound clips. Descriptive statistics were used to summarize the data.
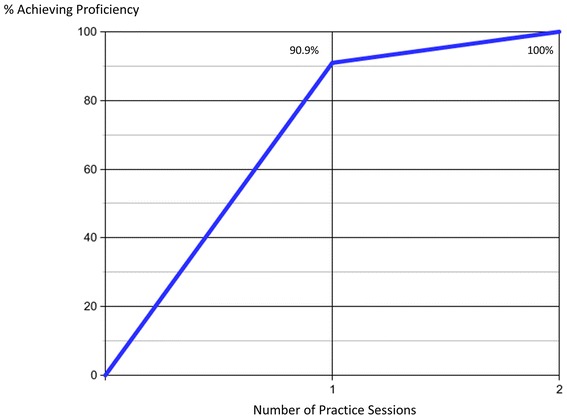
Results: Of the 87 eligible physicians, 66 (75.9 %) completed the study. The mean score on the baseline test was 42.9 % (SD 32.7 %). After the tutorial, 90.9 % (60/66) of the participants achieved proficiency after one practice attempt and 100 % achieved proficiency after two practice attempts. Six intubation ultrasound clips were misinterpreted, for a total error rate of 0.9 % (6/684). Overall, the participants had a sensitivity of 98.3 % (95 % CI 96.3-99.4 %) and specificity of 100 % (95 % CI 98.9-100 %) for detecting correct tube location. Scans were interpreted within an average of 4 s (SD 2.9 s) of the intubation.
Conclusions: After a brief online tutorial and only two practice attempts, emergency physicians were able to quickly and accurately interpret ultrasound intubation clips of esophageal and endotracheal intubations.
背景:未识别的食管插管与显著的患者发病率和死亡率相关。在急诊科,没有单一的确认装置被证明是100%准确地排除食管插管。最近的研究表明,即时超声(POCUS)可能是确认气管内插管放置的有用辅助手段;然而,精通这项技术所需的练习量尚不清楚。本研究的目的是确定急诊医生熟练解读食管和气管插管超声视频片段所需的练习量。方法:急诊医师和急诊住院医师完成基线解释测试,然后进行10分钟的在线教程。然后,他们按随机选择的顺序解释食管和气管插管的POCUS夹。如果给出了不正确的回答,参与者将完成另一个带有反馈的练习环节。这个过程一直持续到他们正确地解读了10个连续的超声波片段。采用描述性统计对数据进行汇总。结果:87名符合条件的医生中,66名(75.9%)完成了研究。基线测试的平均得分为42.9% (SD为32.7%)。辅导结束后,90.9%(60/66)的参与者经过一次练习达到熟练程度,100%的参与者经过两次练习达到熟练程度。6个插管超声夹被误读,总误差率为0.9%(6/684)。总体而言,参与者在检测正确的试管位置方面的敏感性为98.3% (95% CI 96.3- 99.4%),特异性为100% (95% CI 98.9- 100%)。扫描结果在插管后平均4 s (SD 2.9 s)内解释。结论:急诊医师经过简短的在线指导和两次实践尝试后,能够快速准确地解读食管和气管插管超声插管夹。



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
