Daniel Caldeira, Filipe B Rodrigues, Fausto J Pinto, Joaquim J Ferreira, João Costa
{"title":"Thromboprophylaxis With Apixaban in Patients Undergoing Major Orthopedic Surgery: Meta-Analysis and Trial-Sequential Analysis.","authors":"Daniel Caldeira, Filipe B Rodrigues, Fausto J Pinto, Joaquim J Ferreira, João Costa","doi":"10.1177/1179545X17704660","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Venous thromboembolism (VTE) is a potentially fatal complication of orthopedic surgery, and until recently, few antithrombotic compounds were available for postoperative thromboprophylaxis. The introduction of the non-vitamin K antagonists oral anticoagulants (NOAC), including apixaban, has extended the therapeutic armamentarium in this field. Therefore, estimation of NOAC net clinical benefit in comparison with the established treatment is needed to inform clinical decision making.</p><p><strong>Objectives: </strong>Systematic review to assess the efficacy and safety of apixaban 2.5 mg twice a day versus low-molecular-weight heparins (LMWH) for thromboprophylaxis in patients undergoing knee or hip replacement.</p><p><strong>Data sources: </strong>MEDLINE, Embase, and CENTRAL were searched from inception to September 2016, other systematic reviews, reference lists, and experts were consulted.</p><p><strong>Study eligibility criteria participants and intervention: </strong>All major orthopedic surgery randomized controlled trials comparing apixaban 2.5 mg twice daily with LMWH, reporting thrombotic and bleeding events.</p><p><strong>Data extraction: </strong>Two independent reviewers, using a predetermined form.</p><p><strong>Study appraisal and synthesis methods: </strong>The Cochrane tool to assess risk bias was used by two independent authors. RevMan software was used to estimate pooled risk ratio (RR) and 95% confidence intervals (95% CI) using random-effects meta-analysis. Trial sequential analysis (TSA) was performed in statistical significant results to evaluate whether cumulative sample size was powered for the obtained effect. Overall confidence in cumulative evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group methodology.</p><p><strong>Results: </strong>Four studies comparing apixaban 2.5 mg twice daily with LMWH were included, with a total of 11.828 patients (55% undergoing knee and 45% hip replacement). The overall risk of bias across studies was low. In comparison with LMWH (all regimens), apixaban showed a significantly lower risk of VTE events and overall mortality combined (RR: 0.63, 95% CI: 0.42-0.95, <i>I</i>2 = 84%, n = 8346), but not of major VTE events (RR: 0.62, 95% CI: 0.32-1.19, <i>I</i>2 = 63%, n = 9493), or of symptomatic VTE events and VTE-related mortality combined (RR: 1.14, 95% CI: 0.68-1.90, <i>I</i>2 = 0%, n = 11 879). Trial sequential analysis showed that the risk reduction obtained for VTE and mortality was based on underpowered cumulative sample size and effect dimension. Subgroup analysis according to LMWH regimens showed that apixaban reduced the risk of VTE events and overall mortality, and major VTE events, when compared with LMWH once daily, without differences between apixaban and LMWH twice daily.</p><p><strong>Conclusions: </strong>There is low to moderate evidence that in patients undergoing knee or hip replacement, apixaban seems equally effective and safe to LMWH twice a day. When compared with LMWH once a day, apixaban seems a superior thromboprophylaxis option. However, the results are underpowered which precludes definite answers regarding the true net clinical benefit of apixaban versus LMWH in this clinical context.</p>","PeriodicalId":43083,"journal":{"name":"Clinical Medicine Insights-Blood Disorders","volume":"10 ","pages":"1179545X17704660"},"PeriodicalIF":3.0000,"publicationDate":"2017-05-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1179545X17704660","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine Insights-Blood Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1179545X17704660","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 8
Abstract
Background: Venous thromboembolism (VTE) is a potentially fatal complication of orthopedic surgery, and until recently, few antithrombotic compounds were available for postoperative thromboprophylaxis. The introduction of the non-vitamin K antagonists oral anticoagulants (NOAC), including apixaban, has extended the therapeutic armamentarium in this field. Therefore, estimation of NOAC net clinical benefit in comparison with the established treatment is needed to inform clinical decision making.
Objectives: Systematic review to assess the efficacy and safety of apixaban 2.5 mg twice a day versus low-molecular-weight heparins (LMWH) for thromboprophylaxis in patients undergoing knee or hip replacement.
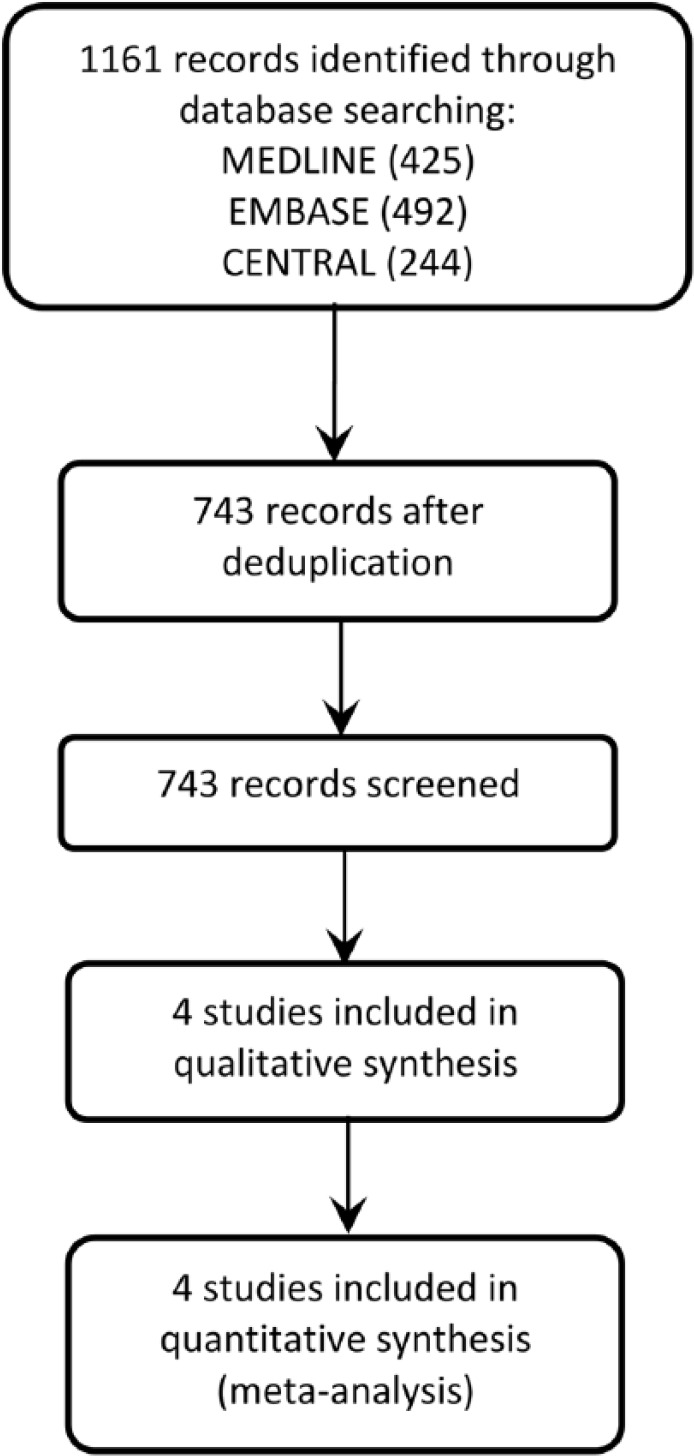
Data sources: MEDLINE, Embase, and CENTRAL were searched from inception to September 2016, other systematic reviews, reference lists, and experts were consulted.
Study eligibility criteria participants and intervention: All major orthopedic surgery randomized controlled trials comparing apixaban 2.5 mg twice daily with LMWH, reporting thrombotic and bleeding events.
Data extraction: Two independent reviewers, using a predetermined form.
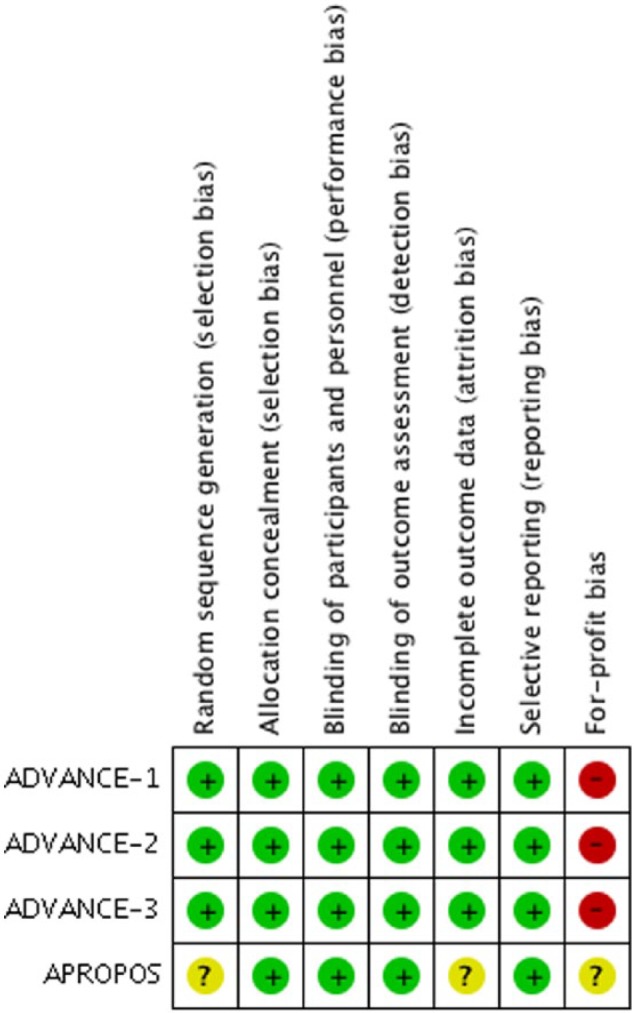
Study appraisal and synthesis methods: The Cochrane tool to assess risk bias was used by two independent authors. RevMan software was used to estimate pooled risk ratio (RR) and 95% confidence intervals (95% CI) using random-effects meta-analysis. Trial sequential analysis (TSA) was performed in statistical significant results to evaluate whether cumulative sample size was powered for the obtained effect. Overall confidence in cumulative evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Working Group methodology.
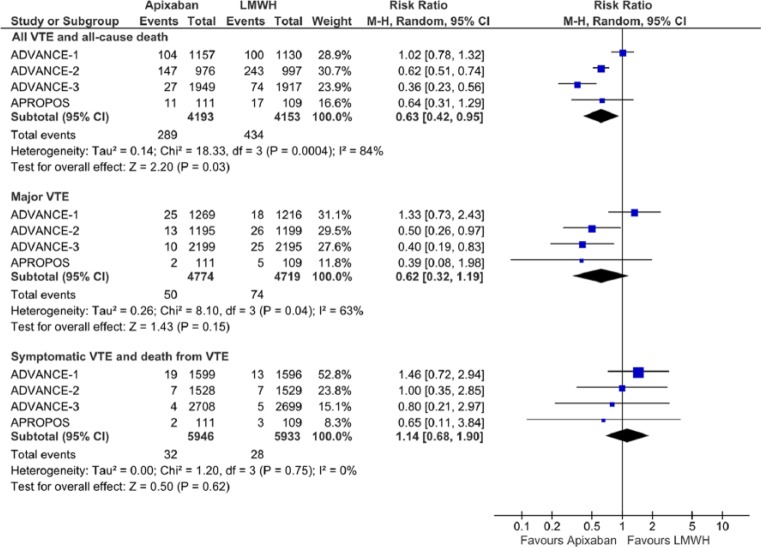
Results: Four studies comparing apixaban 2.5 mg twice daily with LMWH were included, with a total of 11.828 patients (55% undergoing knee and 45% hip replacement). The overall risk of bias across studies was low. In comparison with LMWH (all regimens), apixaban showed a significantly lower risk of VTE events and overall mortality combined (RR: 0.63, 95% CI: 0.42-0.95, I2 = 84%, n = 8346), but not of major VTE events (RR: 0.62, 95% CI: 0.32-1.19, I2 = 63%, n = 9493), or of symptomatic VTE events and VTE-related mortality combined (RR: 1.14, 95% CI: 0.68-1.90, I2 = 0%, n = 11 879). Trial sequential analysis showed that the risk reduction obtained for VTE and mortality was based on underpowered cumulative sample size and effect dimension. Subgroup analysis according to LMWH regimens showed that apixaban reduced the risk of VTE events and overall mortality, and major VTE events, when compared with LMWH once daily, without differences between apixaban and LMWH twice daily.
Conclusions: There is low to moderate evidence that in patients undergoing knee or hip replacement, apixaban seems equally effective and safe to LMWH twice a day. When compared with LMWH once a day, apixaban seems a superior thromboprophylaxis option. However, the results are underpowered which precludes definite answers regarding the true net clinical benefit of apixaban versus LMWH in this clinical context.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
