Evolution and Critics on "Capnography as an Aid in Localizing the Phrenic Nerve in Brachial Plexus Surgery. Technical Note" by Combined Ventilator Waveforms Analysis.
George Georgoulis, Eirini Papagrigoriou, Marc Sindou
{"title":"Evolution and Critics on \"Capnography as an Aid in Localizing the Phrenic Nerve in Brachial Plexus Surgery. Technical Note\" by Combined Ventilator Waveforms Analysis.","authors":"George Georgoulis, Eirini Papagrigoriou, Marc Sindou","doi":"10.1055/s-0037-1608623","DOIUrl":null,"url":null,"abstract":"Dear Editor, We have recently published a work on the intraoperative identification of fourth cervical (C4) root and phrenic nerve during “difficult” surgery, by changing the ventilator waveforms triggered by electrical stimulation of these anatomic structures.1,2 Reviewing the literature on the domain, we came across the correspondence by Bhakta (October 2008) regarding the article “Capnography as an aid in localizing the phrenic nerve in brachial plexus surgery. Technical note.”3,4 Having studied the method in a series of 12 patients for C4 root (microsurgical cervical DREZotomy for neuropathic pain after brachial plexus avulsion) and 2 patients for phrenic nerve (transversomegaly of seventh cervical vertebra and brachial plexus tumor), we would like to add our own findings and conclusions in the discussion. In the original article (May 2008), Bhagat et al4 had presentedtheirwork inwhich thechangesoncapnographyelicited byelectrical stimulationof thephrenicnervehadbeen successfully used for the intraoperative identification of the nerve in a series of threepatients. InOctober2008, Bhaktaquestioned the correlation between the changes on capnography and the stimulation, suggesting that various anesthesiologic parameters could have resulted in similar changes. Our own method consists of the combined analysis of capnography and at least one of pressure–time and flow– time curves. In our series, general intravenous anesthesia was used, without neuromuscular blocking agents. As opposed to thepatients in the series ofBhagat et al,where a laryngealmask was used,4 our patients were intubated and ventilated in fully controlledventilationmodeswith tidal volumes of 6mL/kg and frequencies between 11 and 15. No difference of performance was observed between volume control and pressure control modes. No hyperventilation or air leak around the cuff was suspected at any point. No poststimulation hemodynamic variabilitywas observed. The electrical stimulationwas always performed at around 1 mA. Under these fully controlled conditions, capnography showed a sensitivity of 100% in the detection of the stimulation of either C4 root or phrenic nerve. The disadvantages of the capnography curve alone are that it can only be interpreted during expiration, as values during inspiration are zero, and there is normal delay between the occurrence of ventilatory events and their appearance on the curve. The combined analysis of the three curves offered valuable additional information, thus increasing the specificity of the findings. The study of pressure and flow curves, which are real-time curves covering the entire respiratory cycle, allowed us to confirm the on–off effect, that is, the appearance and disappearance of the changes concomitantly with the onset and end of stimulation. The patterns observed on capnography were of greater amplitude but rather nonspecific, whereas those observed on pressure and/or flow curve were generally of smaller amplitude but more specific, often resembling miniature respiratory cycles. Yet the key feature was that the patterns on pressure and/or flow curves were repetitive, although not always uniform, corresponding to the frequency of the stimulation. This was not so obvious on","PeriodicalId":15280,"journal":{"name":"Journal of Brachial Plexus and Peripheral Nerve Injury","volume":"12 1","pages":"e15-e16"},"PeriodicalIF":1.0000,"publicationDate":"2017-10-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/s-0037-1608623","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Brachial Plexus and Peripheral Nerve Injury","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0037-1608623","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
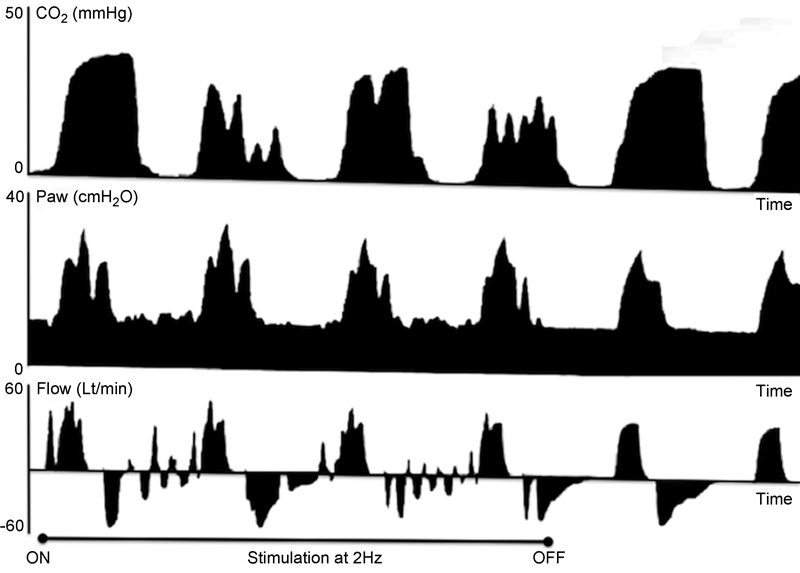
Dear Editor, We have recently published a work on the intraoperative identification of fourth cervical (C4) root and phrenic nerve during “difficult” surgery, by changing the ventilator waveforms triggered by electrical stimulation of these anatomic structures.1,2 Reviewing the literature on the domain, we came across the correspondence by Bhakta (October 2008) regarding the article “Capnography as an aid in localizing the phrenic nerve in brachial plexus surgery. Technical note.”3,4 Having studied the method in a series of 12 patients for C4 root (microsurgical cervical DREZotomy for neuropathic pain after brachial plexus avulsion) and 2 patients for phrenic nerve (transversomegaly of seventh cervical vertebra and brachial plexus tumor), we would like to add our own findings and conclusions in the discussion. In the original article (May 2008), Bhagat et al4 had presentedtheirwork inwhich thechangesoncapnographyelicited byelectrical stimulationof thephrenicnervehadbeen successfully used for the intraoperative identification of the nerve in a series of threepatients. InOctober2008, Bhaktaquestioned the correlation between the changes on capnography and the stimulation, suggesting that various anesthesiologic parameters could have resulted in similar changes. Our own method consists of the combined analysis of capnography and at least one of pressure–time and flow– time curves. In our series, general intravenous anesthesia was used, without neuromuscular blocking agents. As opposed to thepatients in the series ofBhagat et al,where a laryngealmask was used,4 our patients were intubated and ventilated in fully controlledventilationmodeswith tidal volumes of 6mL/kg and frequencies between 11 and 15. No difference of performance was observed between volume control and pressure control modes. No hyperventilation or air leak around the cuff was suspected at any point. No poststimulation hemodynamic variabilitywas observed. The electrical stimulationwas always performed at around 1 mA. Under these fully controlled conditions, capnography showed a sensitivity of 100% in the detection of the stimulation of either C4 root or phrenic nerve. The disadvantages of the capnography curve alone are that it can only be interpreted during expiration, as values during inspiration are zero, and there is normal delay between the occurrence of ventilatory events and their appearance on the curve. The combined analysis of the three curves offered valuable additional information, thus increasing the specificity of the findings. The study of pressure and flow curves, which are real-time curves covering the entire respiratory cycle, allowed us to confirm the on–off effect, that is, the appearance and disappearance of the changes concomitantly with the onset and end of stimulation. The patterns observed on capnography were of greater amplitude but rather nonspecific, whereas those observed on pressure and/or flow curve were generally of smaller amplitude but more specific, often resembling miniature respiratory cycles. Yet the key feature was that the patterns on pressure and/or flow curves were repetitive, although not always uniform, corresponding to the frequency of the stimulation. This was not so obvious on
期刊介绍:
JBPPNI is an open access, peer-reviewed online journal that will encompass all aspects of basic and clinical research findings, in the area of brachial plexus and peripheral nerve injury. Injury in this context refers to congenital, inflammatory, traumatic, degenerative and neoplastic processes, including neurofibromatosis. Papers on diagnostic and imaging aspects of the peripheral nervous system are welcomed as well. The peripheral nervous system is unique in its complexity and scope of influence. There are areas of interest in the anatomy, physiology, metabolism, phylogeny, and limb growth tropism of peripheral nerves.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
