The relationship between single and two-dimensional indices of left ventricular size using hemodynamic transesophageal echocardiography in trauma and burn patients.
Duraid Younan, T Mark Beasley, David C Pigott, C Blayke Gibson, John P Gullett, Jeffrey Richey, Jean-Francois Pittet, Ahmed Zaky
{"title":"The relationship between single and two-dimensional indices of left ventricular size using hemodynamic transesophageal echocardiography in trauma and burn patients.","authors":"Duraid Younan, T Mark Beasley, David C Pigott, C Blayke Gibson, John P Gullett, Jeffrey Richey, Jean-Francois Pittet, Ahmed Zaky","doi":"10.1186/s13089-017-0074-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Conventional echocardiographic technique for assessment of volume status and cardiac contractility utilizes left ventricular end-diastolic area (LVEDA) and fractional area of change (FAC), respectively. Our goal was to find a technically reliable yet faster technique to evaluate volume status and contractility by measuring left ventricular end-diastolic diameter (LVEDD) and fractional shortening (FS) in a cohort of mechanically ventilated trauma and burn patients using hemodynamic transesophageal echocardiographic (hTEE) monitoring.</p><p><strong>Methods: </strong>Retrospective chart review performed at trauma/burn intensive care unit (TBICU). Data on 88 mechanically ventilated surgical intensive care patients cared for between July 2013 and July 2015 were reviewed. Initial measurements of LVEDA, left ventricular end-systolic area (LVESA) and FAC were collected. Post-processing left ventricular end-systolic (LVESD) and end-diastolic diameters (LVEDD) were measured and fractional shortening (FS) was calculated. Two orthogonal measurements of LV diameter were obtained in transverse (Tr) and posteroanterior (PA) orientation.</p><p><strong>Results: </strong>There was a significant correlation between transverse and posteroanterior left ventricular diameter measurements in both systole and diastole. In systole, r = 0.92, p < 0.01 for LVESD-Tr (mean 23.47 mm, SD ± 6.77) and LVESD-PA (mean 24.84 mm, SD = 8.23). In diastole, r = 0.80, p < 0.01 for LVEDD-Tr (mean 37.60 mm, SD ± 6.45), and LVEDD-PA diameters (mean 42.24 mm, SD ± 7.97). Left ventricular area (LVEDA) also significantly correlated with left ventricular diameter LVEDD-Tr (r = 0.84, p < 0.01) and LVEDD-PA (r = 0.90, p < 0.01). Both transverse and PA measurements of fractional shortening were significantly (p < 0.0001) and similarly correlated with systolic function as measured by FAC. Bland-Altman analyses also indicated that the assessment of fractional shortening using left ventricular posteroanterior diameter measurement shows agreement with FAC.</p><p><strong>Conclusions: </strong>Left ventricular diameter measurements are a reliable and technically feasible alternative to left ventricular area measurements in the assessment of cardiac filling and systolic function.</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"9 1","pages":"20"},"PeriodicalIF":3.6000,"publicationDate":"2017-10-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-017-0074-z","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-017-0074-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
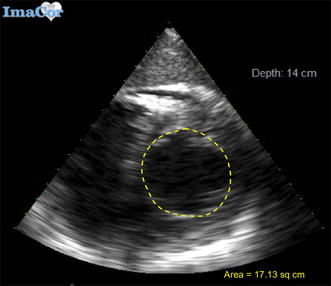
Background: Conventional echocardiographic technique for assessment of volume status and cardiac contractility utilizes left ventricular end-diastolic area (LVEDA) and fractional area of change (FAC), respectively. Our goal was to find a technically reliable yet faster technique to evaluate volume status and contractility by measuring left ventricular end-diastolic diameter (LVEDD) and fractional shortening (FS) in a cohort of mechanically ventilated trauma and burn patients using hemodynamic transesophageal echocardiographic (hTEE) monitoring.
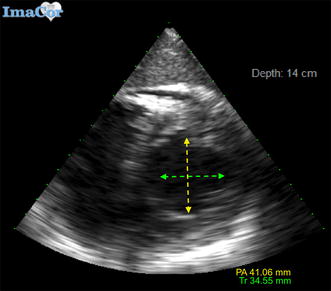
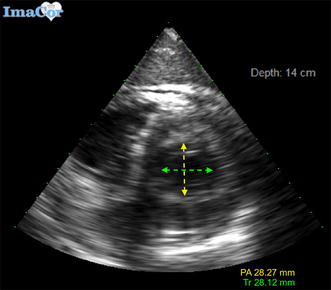
Methods: Retrospective chart review performed at trauma/burn intensive care unit (TBICU). Data on 88 mechanically ventilated surgical intensive care patients cared for between July 2013 and July 2015 were reviewed. Initial measurements of LVEDA, left ventricular end-systolic area (LVESA) and FAC were collected. Post-processing left ventricular end-systolic (LVESD) and end-diastolic diameters (LVEDD) were measured and fractional shortening (FS) was calculated. Two orthogonal measurements of LV diameter were obtained in transverse (Tr) and posteroanterior (PA) orientation.
Results: There was a significant correlation between transverse and posteroanterior left ventricular diameter measurements in both systole and diastole. In systole, r = 0.92, p < 0.01 for LVESD-Tr (mean 23.47 mm, SD ± 6.77) and LVESD-PA (mean 24.84 mm, SD = 8.23). In diastole, r = 0.80, p < 0.01 for LVEDD-Tr (mean 37.60 mm, SD ± 6.45), and LVEDD-PA diameters (mean 42.24 mm, SD ± 7.97). Left ventricular area (LVEDA) also significantly correlated with left ventricular diameter LVEDD-Tr (r = 0.84, p < 0.01) and LVEDD-PA (r = 0.90, p < 0.01). Both transverse and PA measurements of fractional shortening were significantly (p < 0.0001) and similarly correlated with systolic function as measured by FAC. Bland-Altman analyses also indicated that the assessment of fractional shortening using left ventricular posteroanterior diameter measurement shows agreement with FAC.
Conclusions: Left ventricular diameter measurements are a reliable and technically feasible alternative to left ventricular area measurements in the assessment of cardiac filling and systolic function.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
