Analysis of Risk Factors for Kidney Retransplant Outcomes Associated with Common Induction Regimens: A Study of over Twelve-Thousand Cases in the United States.
{"title":"Analysis of Risk Factors for Kidney Retransplant Outcomes Associated with Common Induction Regimens: A Study of over Twelve-Thousand Cases in the United States.","authors":"Alfonso H Santos, Michael J Casey, Karl L Womer","doi":"10.1155/2017/8132672","DOIUrl":null,"url":null,"abstract":"<p><p>We studied registry data of 12,944 adult kidney retransplant recipients categorized by induction regimen received into antithymocyte globulin (ATG) (<i>N</i> = 9120), alemtuzumab (<i>N</i> = 1687), and basiliximab (<i>N</i> = 2137) cohorts. We analyzed risk factors for 1-year acute rejection (AR) and 5-year death-censored graft loss (DCGL) and patient death. Compared with the reference, basiliximab: (1) one-year AR risk was lower with ATG in retransplant recipients of expanded criteria deceased-donor kidneys (HR = 0.56, 95% CI = 0.35-0.91 and HR = 0.54, 95% CI = 0.27-1.08, resp.), while AR risk was lower with alemtuzumab in retransplant recipients with >3 HLA mismatches before transplant (HR = 0.63, 95% CI = 0.44-0.93 and HR = 0.81, 95% CI = 0.63-1.06, resp.); (2) five-year DCGL risk was lower with alemtuzumab, not ATG, in retransplant recipients of African American race (HR = 0.54, 95% CI = 0.34-0.86 and HR = 0.73, 95% CI = 0.51-1.04, resp.) or with pretransplant glomerulonephritis (HR = 0.65, 95% CI = 0.43-0.98 and HR = 0.82, 95% CI = 0.60-1.12, resp.). Therefore, specific risk factor-induction regimen combinations may predict outcomes and this information may help in individualizing induction in retransplant recipients.</p>","PeriodicalId":45795,"journal":{"name":"Journal of Transplantation","volume":"2017 ","pages":"8132672"},"PeriodicalIF":2.2000,"publicationDate":"2017-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5632904/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2017/8132672","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/9/24 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
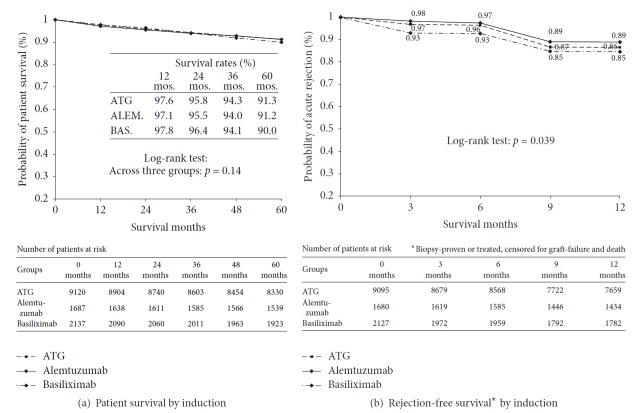
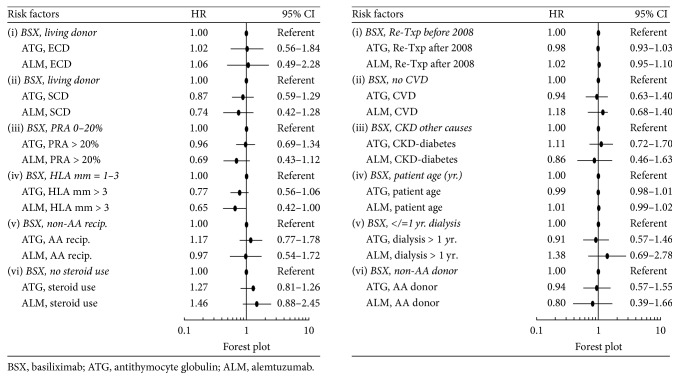
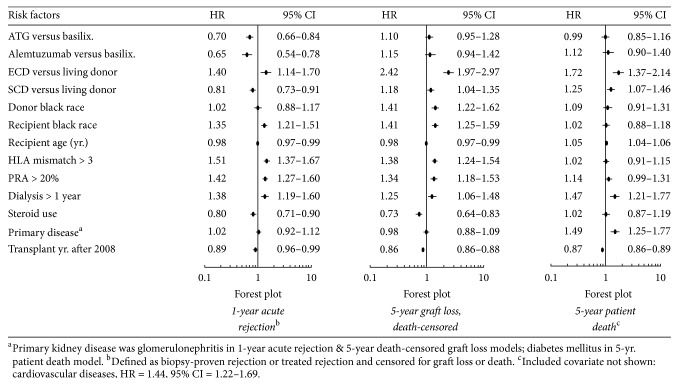
We studied registry data of 12,944 adult kidney retransplant recipients categorized by induction regimen received into antithymocyte globulin (ATG) (N = 9120), alemtuzumab (N = 1687), and basiliximab (N = 2137) cohorts. We analyzed risk factors for 1-year acute rejection (AR) and 5-year death-censored graft loss (DCGL) and patient death. Compared with the reference, basiliximab: (1) one-year AR risk was lower with ATG in retransplant recipients of expanded criteria deceased-donor kidneys (HR = 0.56, 95% CI = 0.35-0.91 and HR = 0.54, 95% CI = 0.27-1.08, resp.), while AR risk was lower with alemtuzumab in retransplant recipients with >3 HLA mismatches before transplant (HR = 0.63, 95% CI = 0.44-0.93 and HR = 0.81, 95% CI = 0.63-1.06, resp.); (2) five-year DCGL risk was lower with alemtuzumab, not ATG, in retransplant recipients of African American race (HR = 0.54, 95% CI = 0.34-0.86 and HR = 0.73, 95% CI = 0.51-1.04, resp.) or with pretransplant glomerulonephritis (HR = 0.65, 95% CI = 0.43-0.98 and HR = 0.82, 95% CI = 0.60-1.12, resp.). Therefore, specific risk factor-induction regimen combinations may predict outcomes and this information may help in individualizing induction in retransplant recipients.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
