{"title":"Nail psoriasis: clinical features, pathogenesis, differential diagnoses, and management.","authors":"Eckart Haneke","doi":"10.2147/PTT.S126281","DOIUrl":null,"url":null,"abstract":"<p><p>Psoriasis is the skin disease that most frequently affects the nails. Depending on the very nail structure involved, different clinical nail alterations can be observed. Irritation of the apical matrix results in psoriatic pits, mid-matrix involvement may cause leukonychia, whole matrix affection may lead to red lunulae or severe nail dystrophy, nail bed involvement may cause salmon spots, subungual hyperkeratosis, and splinter hemorrhages, and psoriasis of the distal nail bed and hyponychium causes onycholysis whereas that of the proximal nail fold causes psoriatic paronychia. The more extensive the involvement, the more severe is the nail destruction. Pustular psoriasis may be seen as yellow spots under the nail or, in case of acrodermatitis continua suppurativa, as an insidious progressive loss of the nail organ. Nail psoriasis has a severe impact on quality of life and may interfere with professional and other activities. Management includes patient counseling, avoidance of stress and strain to the nail apparatus, and different types of treatment. Topical therapy may be tried but is rarely sufficiently efficient. Perilesional injections with corticosteroids and methotrexate are often beneficial but may be painful and cannot be applied to many nails. All systemic treatments clearing widespread skin lesions usually also clear the nail lesions. Recently, biologicals were introduced into nail psoriasis treatment and found to be very effective. However, their use is restricted to severe cases due to high cost and potential systemic adverse effects.</p>","PeriodicalId":74589,"journal":{"name":"Psoriasis (Auckland, N.Z.)","volume":"7 ","pages":"51-63"},"PeriodicalIF":5.2000,"publicationDate":"2017-10-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/PTT.S126281","citationCount":"66","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Psoriasis (Auckland, N.Z.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PTT.S126281","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2017/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 66
Abstract
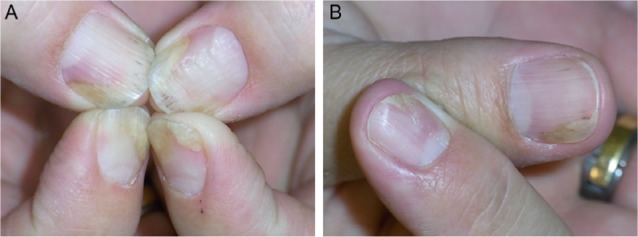
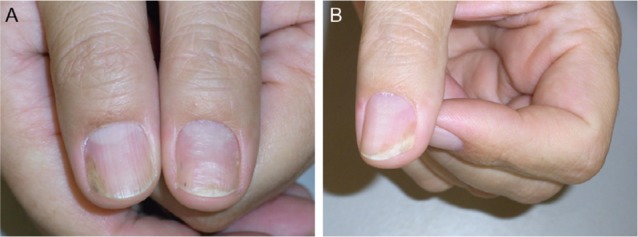
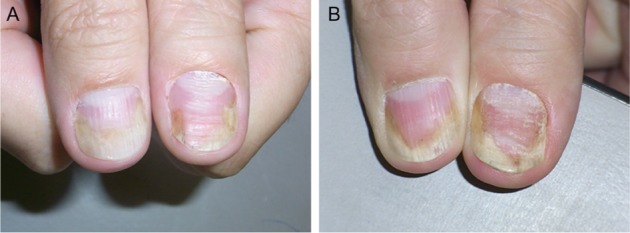
Psoriasis is the skin disease that most frequently affects the nails. Depending on the very nail structure involved, different clinical nail alterations can be observed. Irritation of the apical matrix results in psoriatic pits, mid-matrix involvement may cause leukonychia, whole matrix affection may lead to red lunulae or severe nail dystrophy, nail bed involvement may cause salmon spots, subungual hyperkeratosis, and splinter hemorrhages, and psoriasis of the distal nail bed and hyponychium causes onycholysis whereas that of the proximal nail fold causes psoriatic paronychia. The more extensive the involvement, the more severe is the nail destruction. Pustular psoriasis may be seen as yellow spots under the nail or, in case of acrodermatitis continua suppurativa, as an insidious progressive loss of the nail organ. Nail psoriasis has a severe impact on quality of life and may interfere with professional and other activities. Management includes patient counseling, avoidance of stress and strain to the nail apparatus, and different types of treatment. Topical therapy may be tried but is rarely sufficiently efficient. Perilesional injections with corticosteroids and methotrexate are often beneficial but may be painful and cannot be applied to many nails. All systemic treatments clearing widespread skin lesions usually also clear the nail lesions. Recently, biologicals were introduced into nail psoriasis treatment and found to be very effective. However, their use is restricted to severe cases due to high cost and potential systemic adverse effects.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
