{"title":"Assessing the effectiveness of synthetic and biologic disease-modifying antirheumatic drugs in psoriatic arthritis - a systematic review.","authors":"Gabrielle H Kingsley, David L Scott","doi":"10.2147/PTT.S52893","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Psoriatic arthritis is an inflammatory arthritis the primary manifestations of which are locomotor and skin disease. Although a number of guidelines have been published citing strategies for reducing disease progression, the evidence base for disease-modifying agents is unclear. This forms the focus of this systematic review.</p><p><strong>Methods: </strong>The systematic review was undertaken according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 checklist. We selected randomized controlled trials (RCTs) that looked at the impact of interventions with disease-modifying agents, either synthetic drugs or biologics on musculoskeletal outcomes, notably American College of Rheumatology 20 percent responders. Results were analyzed using Review Manager 5.1.6 (Cochrane Collaboration, Oxford, UK). Whilst our primary focus was on published trials, we also looked at new trials presented in abstract form in 2013-2014 that were not yet published to avoid omitting important and up-to-date information on developing treatments.</p><p><strong>Results: </strong>Our in-depth analysis included 28 trials overall enrolling 5,177 patients published between the 1980s and now as well as limited analysis of some studies in abstract form as described earlier. The most frequently available locomotor outcome measure was the American College of Rheumatology 20 percent responders. The risk ratio for achieving an American College of Rheumatology 20 percent responders response was positive in favor of treatment (risk ratio 2.30; 95% confidence interval 1.78-2.96); however, there was evidence of considerable heterogeneity between trials. Overall randomized controlled trials of established synthetic disease-modifying agents were largely negative (methotrexate, ciclosporin and sulfasalazine) though leflunomide showed a small positive effect. A new synthetic agent, apremilast, did show a positive benefit. For biologics, TNF inhibitors already licensed for use were effective and similar benefits were seen with newer agents including ustekinumab, secukinumab, brodalumab, and abatacept, although the latter did not impact on skin problems. Important limitations of the systematic review included, first, the fact that for many agents there were little data and, second, much of the recent data for newer biologics were only available in abstract form.</p><p><strong>Conclusion: </strong>Conventional disease-modifying agents, with the possible exception of leflunomide, do not show clear evidence of disease-modifying effects in psoriatic arthritis, though a newer synthetic disease-modifying agents, apremilast, appears more effective. Biologic agents appear more beneficial, although more evidence is required for newer agents. This review suggests that it may be necessary to review existing national and international management guidelines for psoriatic arthritis.</p>","PeriodicalId":74589,"journal":{"name":"Psoriasis (Auckland, N.Z.)","volume":"5 ","pages":"71-81"},"PeriodicalIF":5.2000,"publicationDate":"2015-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/PTT.S52893","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Psoriasis (Auckland, N.Z.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PTT.S52893","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2015/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 9
Abstract
Background: Psoriatic arthritis is an inflammatory arthritis the primary manifestations of which are locomotor and skin disease. Although a number of guidelines have been published citing strategies for reducing disease progression, the evidence base for disease-modifying agents is unclear. This forms the focus of this systematic review.
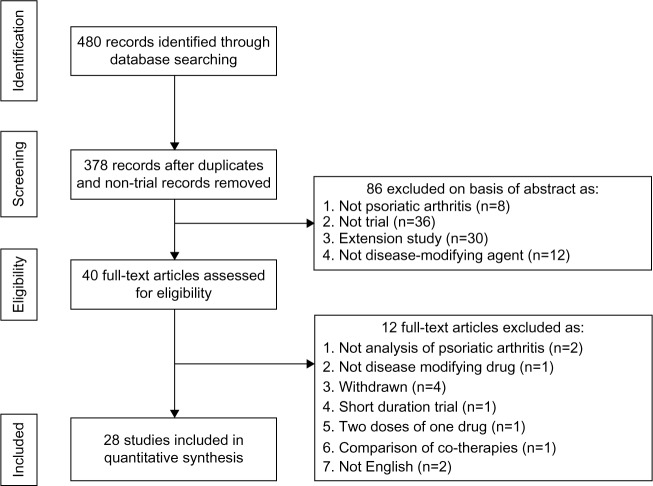
Methods: The systematic review was undertaken according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 checklist. We selected randomized controlled trials (RCTs) that looked at the impact of interventions with disease-modifying agents, either synthetic drugs or biologics on musculoskeletal outcomes, notably American College of Rheumatology 20 percent responders. Results were analyzed using Review Manager 5.1.6 (Cochrane Collaboration, Oxford, UK). Whilst our primary focus was on published trials, we also looked at new trials presented in abstract form in 2013-2014 that were not yet published to avoid omitting important and up-to-date information on developing treatments.
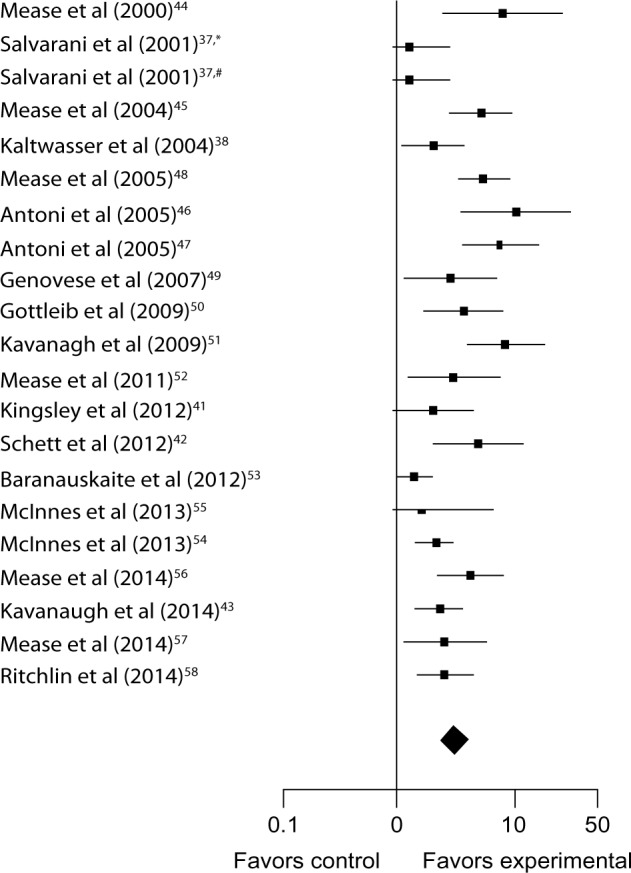
Results: Our in-depth analysis included 28 trials overall enrolling 5,177 patients published between the 1980s and now as well as limited analysis of some studies in abstract form as described earlier. The most frequently available locomotor outcome measure was the American College of Rheumatology 20 percent responders. The risk ratio for achieving an American College of Rheumatology 20 percent responders response was positive in favor of treatment (risk ratio 2.30; 95% confidence interval 1.78-2.96); however, there was evidence of considerable heterogeneity between trials. Overall randomized controlled trials of established synthetic disease-modifying agents were largely negative (methotrexate, ciclosporin and sulfasalazine) though leflunomide showed a small positive effect. A new synthetic agent, apremilast, did show a positive benefit. For biologics, TNF inhibitors already licensed for use were effective and similar benefits were seen with newer agents including ustekinumab, secukinumab, brodalumab, and abatacept, although the latter did not impact on skin problems. Important limitations of the systematic review included, first, the fact that for many agents there were little data and, second, much of the recent data for newer biologics were only available in abstract form.
Conclusion: Conventional disease-modifying agents, with the possible exception of leflunomide, do not show clear evidence of disease-modifying effects in psoriatic arthritis, though a newer synthetic disease-modifying agents, apremilast, appears more effective. Biologic agents appear more beneficial, although more evidence is required for newer agents. This review suggests that it may be necessary to review existing national and international management guidelines for psoriatic arthritis.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
