{"title":"Psoriasis and smoking: links and risks.","authors":"Luigi Naldi","doi":"10.2147/PTT.S85189","DOIUrl":null,"url":null,"abstract":"<p><p>Smoking is a complex environmental exposure influenced by genetic, environmental, and social factors. Nicotine is the principal alkaloid in tobacco that mediates the addicting effects of tobacco products. Tobacco is a mixture of more than 7,000 chemicals, and smoking is recognized as a risk factor for many diseases in humans, including cardiovascular and pulmonary disease and several cancers, and is the single most preventable cause of mortality worldwide. A number of inflammatory immune-related conditions have been associated with smoking, including psoriasis. Smoking affects the onset of psoriasis. In a pooled analysis of 25 case-control studies, the odds ratio of psoriasis among smokers was 1.78 (95% confidence interval [CI]: 1.53-2.06). A dose-effect relationship is also documented. In a pooled analysis of three cohort studies, the risk of incident psoriasis was 1.81 (95% CI: 1.38-2.36) in those who smoked 1-14 cigarettes per day, and 2.29 (95% CI: 1.74-3.01) in those who smoked ≥25 cigarettes per day. Smoking also impacts on the clinical severity of psoriasis, its response to treatment, and explains some of the associated comorbidities, eg, cardiovascular disease, inflammatory bowel disease, and several cancers (especially those of the respiratory tract). Data on the role of smoking in psoriatic arthritis are less consistent compared with those concerning psoriasis. Several pathophysiological mechanisms may explain the association of psoriasis with smoking, including oxidative stress, interaction with signaling pathways active in psoriasis, and vascular influences. In conclusion, psoriasis is just one of the many diseases associated with smoking, but it is visible and disabling. Dermatologists could play a major role in reducing the health burden of smoking by influencing the patients to change their behavior.</p>","PeriodicalId":74589,"journal":{"name":"Psoriasis (Auckland, N.Z.)","volume":"6 ","pages":"65-71"},"PeriodicalIF":5.2000,"publicationDate":"2016-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/PTT.S85189","citationCount":"61","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Psoriasis (Auckland, N.Z.)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/PTT.S85189","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2016/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 61
Abstract
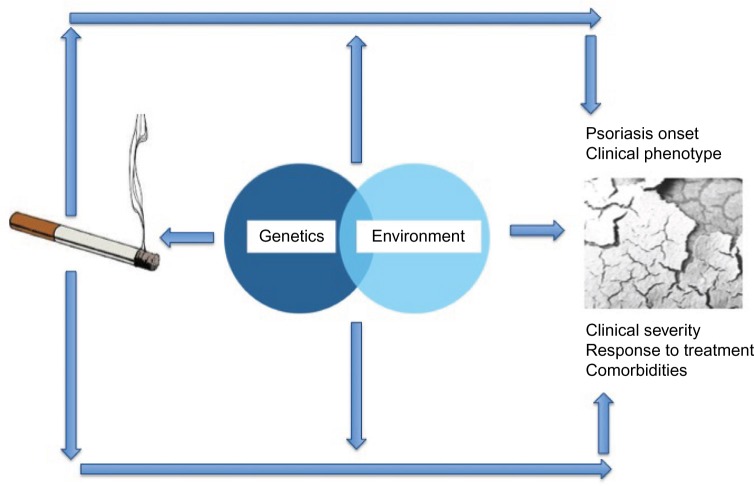
Smoking is a complex environmental exposure influenced by genetic, environmental, and social factors. Nicotine is the principal alkaloid in tobacco that mediates the addicting effects of tobacco products. Tobacco is a mixture of more than 7,000 chemicals, and smoking is recognized as a risk factor for many diseases in humans, including cardiovascular and pulmonary disease and several cancers, and is the single most preventable cause of mortality worldwide. A number of inflammatory immune-related conditions have been associated with smoking, including psoriasis. Smoking affects the onset of psoriasis. In a pooled analysis of 25 case-control studies, the odds ratio of psoriasis among smokers was 1.78 (95% confidence interval [CI]: 1.53-2.06). A dose-effect relationship is also documented. In a pooled analysis of three cohort studies, the risk of incident psoriasis was 1.81 (95% CI: 1.38-2.36) in those who smoked 1-14 cigarettes per day, and 2.29 (95% CI: 1.74-3.01) in those who smoked ≥25 cigarettes per day. Smoking also impacts on the clinical severity of psoriasis, its response to treatment, and explains some of the associated comorbidities, eg, cardiovascular disease, inflammatory bowel disease, and several cancers (especially those of the respiratory tract). Data on the role of smoking in psoriatic arthritis are less consistent compared with those concerning psoriasis. Several pathophysiological mechanisms may explain the association of psoriasis with smoking, including oxidative stress, interaction with signaling pathways active in psoriasis, and vascular influences. In conclusion, psoriasis is just one of the many diseases associated with smoking, but it is visible and disabling. Dermatologists could play a major role in reducing the health burden of smoking by influencing the patients to change their behavior.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
