Vinflunine for the treatment of advanced or metastatic transitional cell carcinoma of the urothelial tract: an evidence-based review of safety, efficacy, and place in therapy.
Steven C Brousell, Joseph J Fantony, Megan G Van Noord, Michael R Harrison, Brant A Inman
{"title":"Vinflunine for the treatment of advanced or metastatic transitional cell carcinoma of the urothelial tract: an evidence-based review of safety, efficacy, and place in therapy.","authors":"Steven C Brousell, Joseph J Fantony, Megan G Van Noord, Michael R Harrison, Brant A Inman","doi":"10.2147/CE.S118670","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A systematic review and meta-analysis of the use of systemic vinflunine (VIN) in the treatment of urothelial carcinoma (UC) was performed to evaluate its efficacy based on current available clinical data.</p><p><strong>Methods: </strong>This review was prospectively registered at the International Prospective Register of Systematic Reviews, PROSPERO (registration CRD42016049294). Electronic databases including MEDLINE<sup>®</sup>, Embase<sup>®</sup>, Cochrane Central Register of Controlled Trials, and Web of Science were searched through December 2016. We performed a meta-analysis of the published data. Primary end points were progression-free survival (PFS) and overall survival (OS). Numerous secondary clinical outcomes were analyzed including response and toxicity data.</p><p><strong>Results: </strong>We identified 382 publications, of which 35 met inclusion criteria for this review representing 29 unique studies. A total of 2,255 patients received VIN for the treatment of UC in the included studies. OS and PFS were analyzed in a pooled Kaplan-Meier analysis. Response data were available for 1,416 VIN-treated patients with random effects proportion of complete response in 1%, partial response in 18%, and overall response rate of 21%. Toxicity analysis revealed fatigue (40.1%), nausea (33.9%), constipation (34.1%), and alopecia (26.0%) as the most prevalent overall non-hematologic adverse events (AEs). Most prevalent grade 3-4 AEs were fatigue (10.2%), abdominal pain (8.2%), myalgias (2.5%), and nausea (2.3%). Most common hematologic AEs of all grades were anemia (56.6%), neutropenia (46.0%), thrombocytopenia (25.5%), and febrile neutropenia (6.6%). Grade 3-4 hematologic AEs had the following pooled rates: neutropenia, 24.6%; anemia, 10.2%; febrile neutropenia, 5.4%; and thrombocytopenia, 3.0%.</p><p><strong>Conclusion: </strong>VIN has been explored as a combination first-line treatment as well as a single-agent second-line, third-line, and maintenance therapy for advanced and metastatic UC. In first-line treatment of UC, either as a maintenance agent after cisplatin or as a primary combination therapy, VIN may be a promising alternative to current treatments. Further studies are needed to compare first-line combination VIN regimens to the current standard of care in order to assess long-term survival outcomes. Second- and third-line VIN monotherapy does provide a proven, although limited, survival benefit in platinum-refractory patients.</p>","PeriodicalId":10764,"journal":{"name":"Core Evidence","volume":"13 ","pages":"1-12"},"PeriodicalIF":0.0000,"publicationDate":"2018-01-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/CE.S118670","citationCount":"12","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Core Evidence","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CE.S118670","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 12
Abstract
Background: A systematic review and meta-analysis of the use of systemic vinflunine (VIN) in the treatment of urothelial carcinoma (UC) was performed to evaluate its efficacy based on current available clinical data.
Methods: This review was prospectively registered at the International Prospective Register of Systematic Reviews, PROSPERO (registration CRD42016049294). Electronic databases including MEDLINE®, Embase®, Cochrane Central Register of Controlled Trials, and Web of Science were searched through December 2016. We performed a meta-analysis of the published data. Primary end points were progression-free survival (PFS) and overall survival (OS). Numerous secondary clinical outcomes were analyzed including response and toxicity data.
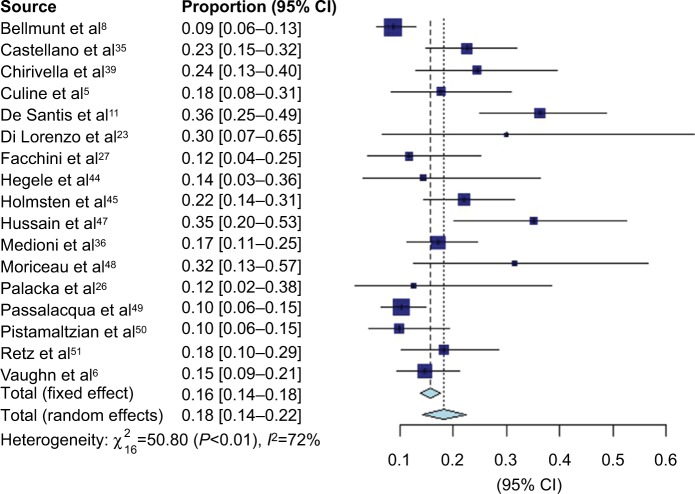
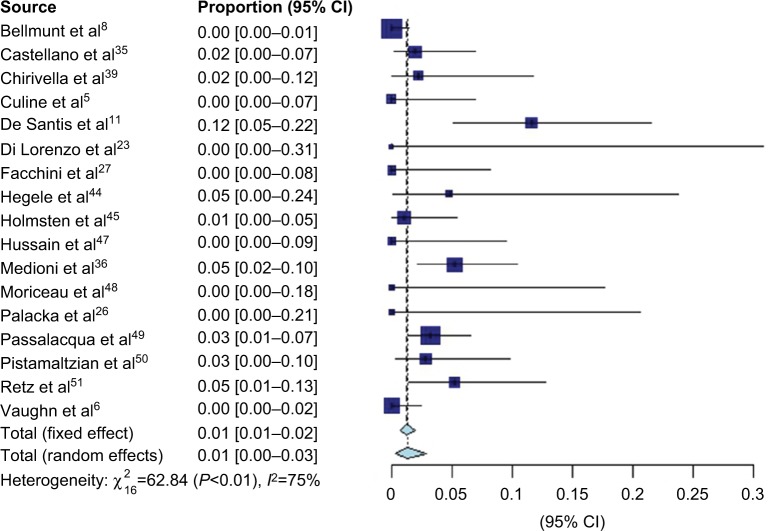
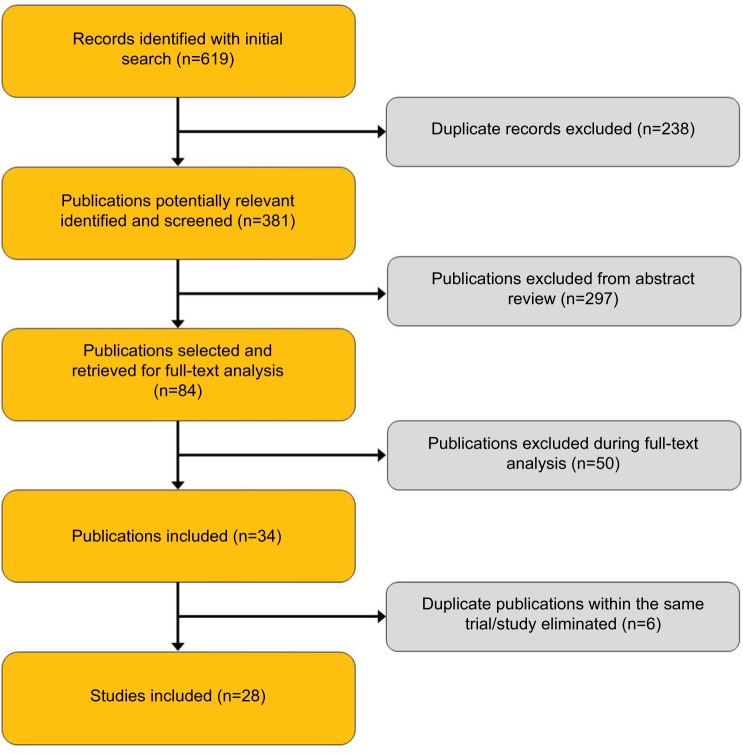
Results: We identified 382 publications, of which 35 met inclusion criteria for this review representing 29 unique studies. A total of 2,255 patients received VIN for the treatment of UC in the included studies. OS and PFS were analyzed in a pooled Kaplan-Meier analysis. Response data were available for 1,416 VIN-treated patients with random effects proportion of complete response in 1%, partial response in 18%, and overall response rate of 21%. Toxicity analysis revealed fatigue (40.1%), nausea (33.9%), constipation (34.1%), and alopecia (26.0%) as the most prevalent overall non-hematologic adverse events (AEs). Most prevalent grade 3-4 AEs were fatigue (10.2%), abdominal pain (8.2%), myalgias (2.5%), and nausea (2.3%). Most common hematologic AEs of all grades were anemia (56.6%), neutropenia (46.0%), thrombocytopenia (25.5%), and febrile neutropenia (6.6%). Grade 3-4 hematologic AEs had the following pooled rates: neutropenia, 24.6%; anemia, 10.2%; febrile neutropenia, 5.4%; and thrombocytopenia, 3.0%.
Conclusion: VIN has been explored as a combination first-line treatment as well as a single-agent second-line, third-line, and maintenance therapy for advanced and metastatic UC. In first-line treatment of UC, either as a maintenance agent after cisplatin or as a primary combination therapy, VIN may be a promising alternative to current treatments. Further studies are needed to compare first-line combination VIN regimens to the current standard of care in order to assess long-term survival outcomes. Second- and third-line VIN monotherapy does provide a proven, although limited, survival benefit in platinum-refractory patients.
背景:根据现有的临床数据,对全身性长春氟宁(VIN)治疗尿路上皮癌(UC)的疗效进行了系统回顾和荟萃分析。方法:本综述在国际前瞻性系统评价注册库PROSPERO进行前瞻性注册(注册号CRD42016049294)。截至2016年12月,检索了MEDLINE®、Embase®、Cochrane Central Register of Controlled Trials和Web of Science等电子数据库。我们对发表的数据进行了荟萃分析。主要终点为无进展生存期(PFS)和总生存期(OS)。分析了许多次要临床结果,包括反应和毒性数据。结果:我们确定了382篇出版物,其中35篇符合本综述的纳入标准,代表29项独特的研究。在纳入的研究中,共有2255名患者接受了VIN治疗UC。OS和PFS采用Kaplan-Meier合并分析。1416例vin治疗患者的反应数据可获得,随机效应比例为完全缓解1%,部分缓解18%,总缓解率21%。毒性分析显示,疲劳(40.1%)、恶心(33.9%)、便秘(34.1%)和脱发(26.0%)是最常见的总体非血液学不良事件(ae)。最常见的3-4级ae是疲劳(10.2%)、腹痛(8.2%)、肌痛(2.5%)和恶心(2.3%)。所有级别最常见的血液学ae是贫血(56.6%)、中性粒细胞减少(46.0%)、血小板减少(25.5%)和发热性中性粒细胞减少(6.6%)。3-4级血液学ae的合并发生率如下:中性粒细胞减少,24.6%;贫血,10.2%;发热性中性粒细胞减少症,5.4%;血小板减少症,3.0%。结论:VIN已被探索作为晚期和转移性UC的一线联合治疗,以及单药二线、三线和维持治疗。在UC的一线治疗中,无论是作为顺铂后的维持剂,还是作为主要的联合治疗,VIN都可能是当前治疗的一个有希望的替代方案。为了评估长期生存结果,需要进一步的研究来比较一线联合VIN方案与目前的标准护理方案。二线和三线VIN单药治疗确实在铂难治患者中提供了已证实的(尽管有限)生存获益。
期刊介绍:
Core Evidence evaluates the evidence underlying the potential place in therapy of drugs throughout their development lifecycle from preclinical to postlaunch. The focus of each review is to evaluate the case for a new drug or class in outcome terms in specific indications and patient groups The emerging evidence on new drugs is reviewed at key stages of development and evaluated against unmet needs



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
