Joe Littlechild, Muneer Junejo, Anne-Marie Simons, Finlay Curran, Darren Subar
{"title":"Emergency resection surgery for colorectal cancer: Patterns of recurrent disease and survival.","authors":"Joe Littlechild, Muneer Junejo, Anne-Marie Simons, Finlay Curran, Darren Subar","doi":"10.4291/wjgp.v9.i1.8","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To evaluate prognostic pathological factors associated with early metachronous disease and adverse long-term survival in these patients.</p><p><strong>Methods: </strong>Clinical and histological features were analysed retrospectively over an eight-year period for prognostic impact on recurrent disease and overall survival in patients undergoing curative resection of a primary colorectal cancer.</p><p><strong>Results: </strong>A total of 266 patients underwent curative surgery during the study period. The median age of the study cohort was 68 year (range 26 to 91) with a follow-up of 7.9 years (range 4.6 to 12.6). Resection was undertaken electively in 225 (84.6%) patients and emergency resection in 35 (13.2%). Data on timing of surgery was missing in 6 patients. Recurrence was noted in 67 (25.2%) during the study period and was predominantly early within 3 years (82.1%) and involved hepatic metastasis in 73.1%. Emergency resection (OR = 3.60, <i>P</i> = 0.001), T4 stage (OR = 4.33, <i>P</i> < 0.001) and lymphovascular invasion (LVI) (OR = 2.37, <i>P</i> = 0.032) were associated with higher risk of recurrent disease. Emergency resection, T4 disease and a high lymph node ratio (LNR) were strong independent predictors of adverse long-term survival.</p><p><strong>Conclusion: </strong>Emergency surgery is associated with adverse disease free and long-term survival. T4 disease, LVI and LNR provide strong independent predictive value of long-term outcome and can inform surveillance strategies to improve outcomes.</p>","PeriodicalId":23760,"journal":{"name":"World Journal of Gastrointestinal Pathophysiology","volume":"9 1","pages":"8-17"},"PeriodicalIF":0.0000,"publicationDate":"2018-02-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/bf/8e/WJGP-9-8.PMC5823701.pdf","citationCount":"10","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Pathophysiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4291/wjgp.v9.i1.8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 10
Abstract
Aim: To evaluate prognostic pathological factors associated with early metachronous disease and adverse long-term survival in these patients.
Methods: Clinical and histological features were analysed retrospectively over an eight-year period for prognostic impact on recurrent disease and overall survival in patients undergoing curative resection of a primary colorectal cancer.
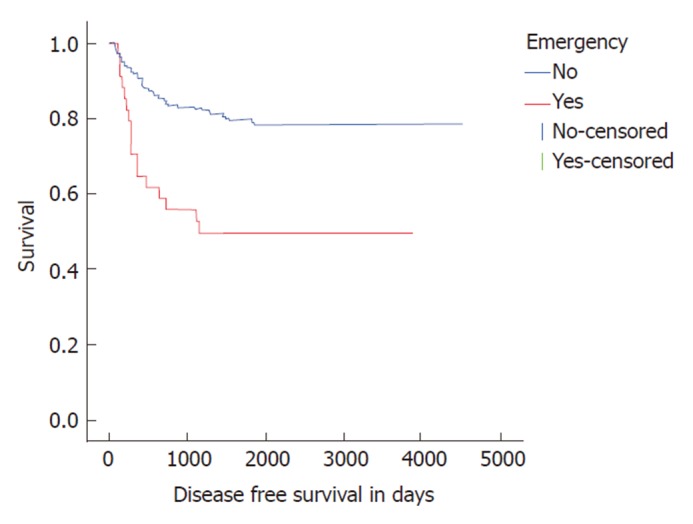
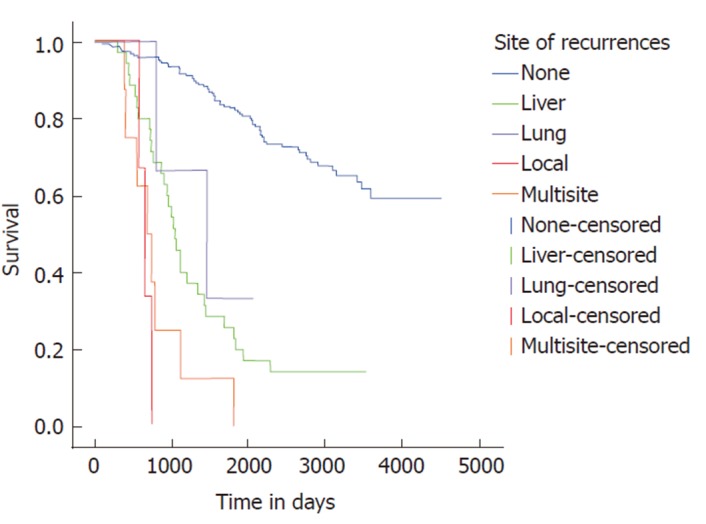
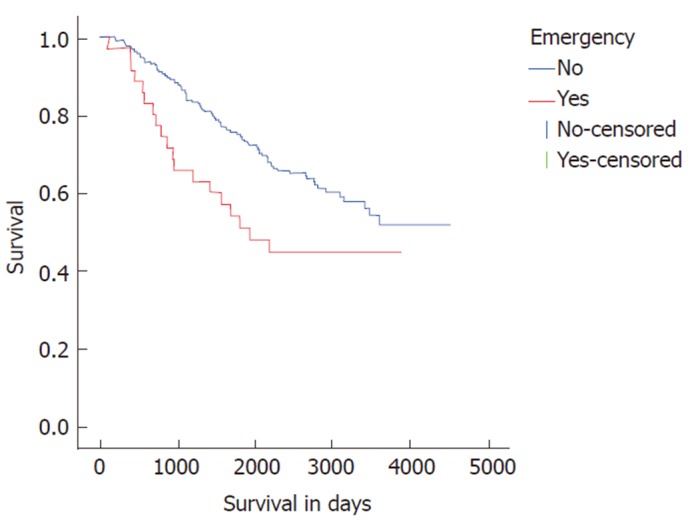
Results: A total of 266 patients underwent curative surgery during the study period. The median age of the study cohort was 68 year (range 26 to 91) with a follow-up of 7.9 years (range 4.6 to 12.6). Resection was undertaken electively in 225 (84.6%) patients and emergency resection in 35 (13.2%). Data on timing of surgery was missing in 6 patients. Recurrence was noted in 67 (25.2%) during the study period and was predominantly early within 3 years (82.1%) and involved hepatic metastasis in 73.1%. Emergency resection (OR = 3.60, P = 0.001), T4 stage (OR = 4.33, P < 0.001) and lymphovascular invasion (LVI) (OR = 2.37, P = 0.032) were associated with higher risk of recurrent disease. Emergency resection, T4 disease and a high lymph node ratio (LNR) were strong independent predictors of adverse long-term survival.
Conclusion: Emergency surgery is associated with adverse disease free and long-term survival. T4 disease, LVI and LNR provide strong independent predictive value of long-term outcome and can inform surveillance strategies to improve outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
