{"title":"Obstructive Sleep Apnea as a Risk Factor for Atrial Fibrillation: A Meta-Analysis.","authors":"Irini Youssef, Haroon Kamran, Mena Yacoub, Nirav Patel, Clive Goulbourne, Shweta Kumar, Jesse Kane, Haley Hoffner, Moro Salifu, Samy I McFarlane","doi":"10.4172/2167-0277.1000282","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To conducted a meta-analysis assessing the relationship between Obstructive Sleep Apnea (OSA) and the risk of Atrial Fibrillation (AF).</p><p><strong>Methods: </strong>We searched PUBMED, Medline, and Cochrane Library using the keywords \"atrial fibrillation\", \"obstructive sleep apnea\" and \"sleep disordered breathing (SDB)\". All subjects included had established diagnosis of OSA/SDB. We then compared the occurrence of AF versus no AF. Analysis done with Comprehensive Meta-Analysis package V3 (Biostat, USA).</p><p><strong>Results: </strong>A total of 579 results were generated. Duplicates were removed and 372 records were excluded based on irrelevant abstracts, titles, study design not consistent with the stated outcome, or full-text unavailable. Twelve studies meeting the inclusion criteria were reviewed in full-text; 2 of these articles were eventually removed due to unconfirmed OSA diagnostic modality, and one was also removed based on a control group inconsistent with the other studies. Therefore, a total of 9 studies were included (n=19,837). Sample sizes ranged from n=160 patients to n=6841 patients. The risk of AF was found to be higher among OSA/SDB versus control group (OR; 2.120, C.I: 1.845-2.436, Z; 10.598 p: <0.001). The heterogeneity observed for the pooled analysis was Q-value; 22.487 df (Q); 8 P-value; 0.004, I-squared; 64.424 Tau2; 0.098, suggesting appropriate study selection and moderate heterogeneity.</p><p><strong>Conclusion: </strong>OSA/SDB is strongly associated with AFib confirming the notion that OSA/SDB populations are high risk for development of AF. Prospective studies are needed to ascertain the effect of the treatment of OSA/SDB for the prevention of AF, a growing health burden with serious consequences.</p>","PeriodicalId":73946,"journal":{"name":"Journal of sleep disorders & therapy","volume":"7 1","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2018-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.4172/2167-0277.1000282","citationCount":"59","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of sleep disorders & therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4172/2167-0277.1000282","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/2/12 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 59
Abstract
Objectives: To conducted a meta-analysis assessing the relationship between Obstructive Sleep Apnea (OSA) and the risk of Atrial Fibrillation (AF).
Methods: We searched PUBMED, Medline, and Cochrane Library using the keywords "atrial fibrillation", "obstructive sleep apnea" and "sleep disordered breathing (SDB)". All subjects included had established diagnosis of OSA/SDB. We then compared the occurrence of AF versus no AF. Analysis done with Comprehensive Meta-Analysis package V3 (Biostat, USA).
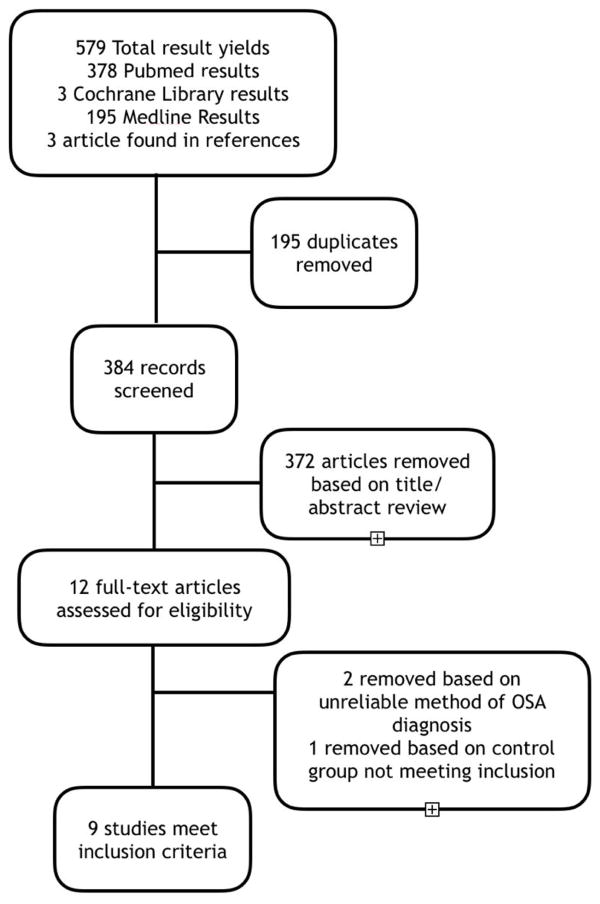
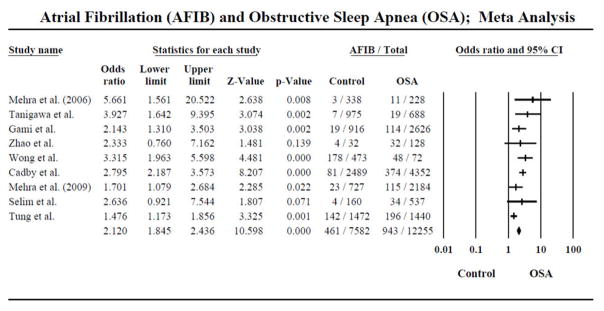
Results: A total of 579 results were generated. Duplicates were removed and 372 records were excluded based on irrelevant abstracts, titles, study design not consistent with the stated outcome, or full-text unavailable. Twelve studies meeting the inclusion criteria were reviewed in full-text; 2 of these articles were eventually removed due to unconfirmed OSA diagnostic modality, and one was also removed based on a control group inconsistent with the other studies. Therefore, a total of 9 studies were included (n=19,837). Sample sizes ranged from n=160 patients to n=6841 patients. The risk of AF was found to be higher among OSA/SDB versus control group (OR; 2.120, C.I: 1.845-2.436, Z; 10.598 p: <0.001). The heterogeneity observed for the pooled analysis was Q-value; 22.487 df (Q); 8 P-value; 0.004, I-squared; 64.424 Tau2; 0.098, suggesting appropriate study selection and moderate heterogeneity.
Conclusion: OSA/SDB is strongly associated with AFib confirming the notion that OSA/SDB populations are high risk for development of AF. Prospective studies are needed to ascertain the effect of the treatment of OSA/SDB for the prevention of AF, a growing health burden with serious consequences.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
