{"title":"Naloxone-Induced Non-Cardiogenic Pulmonary Edema: A Case Report.","authors":"Nasheena Jiwa, Himesh Sheth, Richard Silverman","doi":"10.1007/s40800-018-0088-x","DOIUrl":null,"url":null,"abstract":"<p><p>A 22-year-old man was admitted for an elective right-shoulder open subacromial decompression and distal clavicle excision. He received a single intravenous dose of fentanyl 50 μg for anesthesia. His procedure was completed without intra-operative complications; however, he developed post-operative respiratory depression in the setting of narcotic administration. He was given naloxone 0.2 mg intravenously once to reverse this effect, which subsequently led to acute hypoxic respiratory failure secondary to pulmonary edema shortly after administration of naloxone. His oxygen saturation was noted to be 50% on room air, he was tachypneic with a respiratory rate of 22, and his heart rate ranged from 89 to 104 beats per minute. His blood pressure remained within normal limits at 128/62. His chest X-ray was notable for patchy bilateral perihilar infiltrates and the patient was intubated postoperatively. An EKG revealed normal sinus rhythm, and cardiac enzymes were negative. He was diagnosed with naloxone-induced non-cardiogenic pulmonary edema supported by the temporal relationship of the causal drug and no other identifiable cause of his clinical picture. He received furosemide and underwent diuresis while intubated, with subsequent improvement in his oxygen requirements. His vitals remained stable and he was extubated 6 h later. A Naranjo assessment score of 6 was obtained, indicating a probable relationship between the patient's symptoms and the suspect drug.</p>","PeriodicalId":11364,"journal":{"name":"Drug Safety - Case Reports","volume":"5 1","pages":"20"},"PeriodicalIF":0.0000,"publicationDate":"2018-05-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1007/s40800-018-0088-x","citationCount":"17","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety - Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40800-018-0088-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 17
Abstract
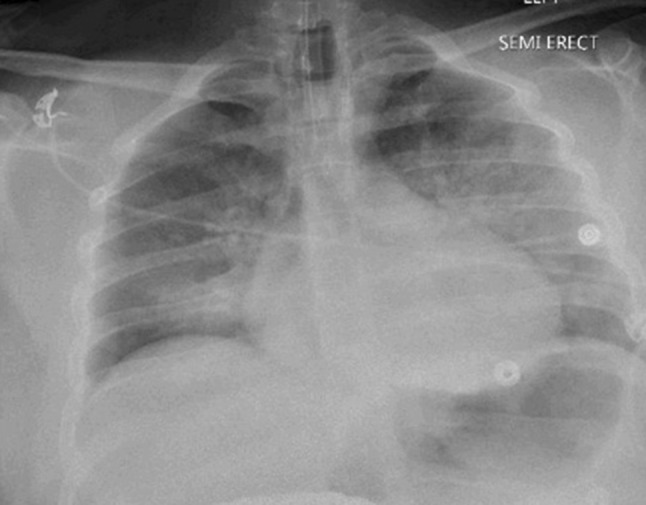
A 22-year-old man was admitted for an elective right-shoulder open subacromial decompression and distal clavicle excision. He received a single intravenous dose of fentanyl 50 μg for anesthesia. His procedure was completed without intra-operative complications; however, he developed post-operative respiratory depression in the setting of narcotic administration. He was given naloxone 0.2 mg intravenously once to reverse this effect, which subsequently led to acute hypoxic respiratory failure secondary to pulmonary edema shortly after administration of naloxone. His oxygen saturation was noted to be 50% on room air, he was tachypneic with a respiratory rate of 22, and his heart rate ranged from 89 to 104 beats per minute. His blood pressure remained within normal limits at 128/62. His chest X-ray was notable for patchy bilateral perihilar infiltrates and the patient was intubated postoperatively. An EKG revealed normal sinus rhythm, and cardiac enzymes were negative. He was diagnosed with naloxone-induced non-cardiogenic pulmonary edema supported by the temporal relationship of the causal drug and no other identifiable cause of his clinical picture. He received furosemide and underwent diuresis while intubated, with subsequent improvement in his oxygen requirements. His vitals remained stable and he was extubated 6 h later. A Naranjo assessment score of 6 was obtained, indicating a probable relationship between the patient's symptoms and the suspect drug.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
