Lara Farhat, Jasmeen Dara, Susan Duberstein, Aliva De
{"title":"Secondary Hypogammaglobulinemia After Rituximab for Neuromyelitis Optica: A Case Report.","authors":"Lara Farhat, Jasmeen Dara, Susan Duberstein, Aliva De","doi":"10.1007/s40800-018-0087-y","DOIUrl":null,"url":null,"abstract":"<p><p>A 17-year-old male with history of neuromyelitis optica and seizures presented to the pulmonology clinic for evaluation of recurrent pneumonias. He had received rituximab for the past 6 years. Over the past 2 years, he experienced four episodes of pneumonia. In between these episodes, he would improve briefly but continued to have daily cough that was productive with yellow phlegm. He also had recurrent rhinitis and sinusitis despite multiple antibiotic courses. Review of chest X-rays revealed localized right middle lobe and right lower lobe infiltrates. An extensive workup was performed, including computed tomography (CT) of the chest and bronchoscopy to rule out congenital lesions of the right lung and foreign body aspiration. Chest CT showed right lower lobe bronchiectasis. Flexible bronchoscopy with bronchoalveolar lavage showed normal anatomy with thick mucus secretions in the right lower lobe. Immunologic evaluation was performed and revealed low levels of immunoglobulin (Ig)-G, IgM, and IgA, which had declined since initiation of rituximab. Lymphocyte subset testing was remarkable for low cluster of differentiation (CD)-19. He was referred to allergy and immunology and was initiated on immunoglobulin-replacement therapy (IGRT) for acquired hypogammaglobulinemia secondary to rituximab. There was marked clinical improvement after initiation of IGRT.</p>","PeriodicalId":11364,"journal":{"name":"Drug Safety - Case Reports","volume":"5 1","pages":"22"},"PeriodicalIF":0.0000,"publicationDate":"2018-05-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/e6/c3/40800_2018_Article_87.PMC5948191.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Safety - Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40800-018-0087-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
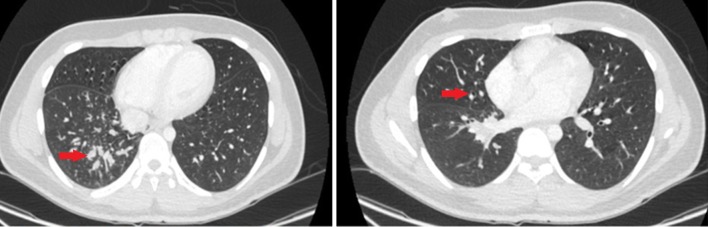
A 17-year-old male with history of neuromyelitis optica and seizures presented to the pulmonology clinic for evaluation of recurrent pneumonias. He had received rituximab for the past 6 years. Over the past 2 years, he experienced four episodes of pneumonia. In between these episodes, he would improve briefly but continued to have daily cough that was productive with yellow phlegm. He also had recurrent rhinitis and sinusitis despite multiple antibiotic courses. Review of chest X-rays revealed localized right middle lobe and right lower lobe infiltrates. An extensive workup was performed, including computed tomography (CT) of the chest and bronchoscopy to rule out congenital lesions of the right lung and foreign body aspiration. Chest CT showed right lower lobe bronchiectasis. Flexible bronchoscopy with bronchoalveolar lavage showed normal anatomy with thick mucus secretions in the right lower lobe. Immunologic evaluation was performed and revealed low levels of immunoglobulin (Ig)-G, IgM, and IgA, which had declined since initiation of rituximab. Lymphocyte subset testing was remarkable for low cluster of differentiation (CD)-19. He was referred to allergy and immunology and was initiated on immunoglobulin-replacement therapy (IGRT) for acquired hypogammaglobulinemia secondary to rituximab. There was marked clinical improvement after initiation of IGRT.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
