Nan Cheng, Heather M Wied, James J Gaul, Lauren E Doyle, Stephen G Reich
{"title":"SCA2 presenting as a focal dystonia.","authors":"Nan Cheng, Heather M Wied, James J Gaul, Lauren E Doyle, Stephen G Reich","doi":"10.1186/s40734-018-0073-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spinocerebellar ataxia 2 (SCA2) is an autosomal dominant neurodegenerative disorder caused by CAG repeat expansions in <i>ATXN2</i> on chromosome 12q24. Patients present with adult-onset progressive gait ataxia, slow saccades, nystagmus, dysarthria and peripheral neuropathy. Dystonia is known to occur as SCA2 advances, but is rarely the presenting symptom.</p><p><strong>Case presentation: </strong>A 43-year-old right handed woman presented with focal dystonia of the right hand which started two years earlier with difficulty writing. There were only mild cerebellar signs. Her mother was reported to have a progressive gait disorder and we subsequently learned that she had SCA2. A total of 10 maternal family members were similarly affected. Over the course of 10 years, the patient's cerebellar signs progressed only mildly however the dystonia worsened to the extent of inability to use her right hand. Dystonia did not improve significantly with botulinum toxin, levodopa or trihexyphenidyl, but has shown marked improvement since DBS implantation in the GPi.</p><p><strong>Conclusions: </strong>We describe a patient with SCA2 who presented with focal dystonia of the right upper extremity. Subtle cerebellar signs as well as the family history became especially important given the absence of predominant gait ataxia. Our case emphasizes that focal dystonia is not only a feature of SCA2, but can also rarely be the presenting sign as well as the most prominent feature during the disease course.</p>","PeriodicalId":15374,"journal":{"name":"Journal of Clinical Movement Disorders","volume":"5 ","pages":"6"},"PeriodicalIF":0.0000,"publicationDate":"2018-08-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40734-018-0073-7","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Movement Disorders","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40734-018-0073-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Spinocerebellar ataxia 2 (SCA2) is an autosomal dominant neurodegenerative disorder caused by CAG repeat expansions in ATXN2 on chromosome 12q24. Patients present with adult-onset progressive gait ataxia, slow saccades, nystagmus, dysarthria and peripheral neuropathy. Dystonia is known to occur as SCA2 advances, but is rarely the presenting symptom.
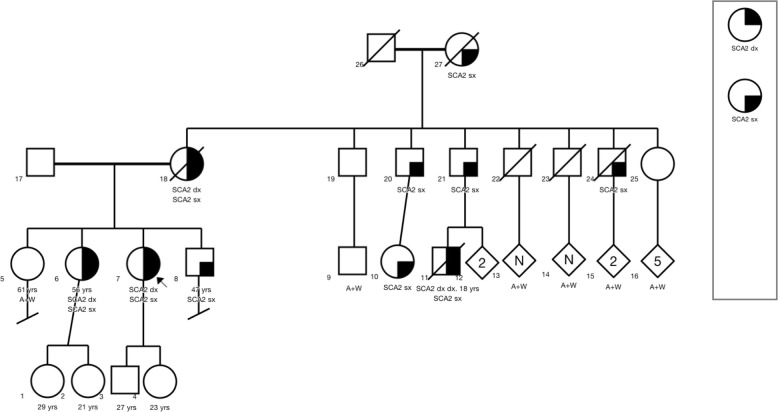
Case presentation: A 43-year-old right handed woman presented with focal dystonia of the right hand which started two years earlier with difficulty writing. There were only mild cerebellar signs. Her mother was reported to have a progressive gait disorder and we subsequently learned that she had SCA2. A total of 10 maternal family members were similarly affected. Over the course of 10 years, the patient's cerebellar signs progressed only mildly however the dystonia worsened to the extent of inability to use her right hand. Dystonia did not improve significantly with botulinum toxin, levodopa or trihexyphenidyl, but has shown marked improvement since DBS implantation in the GPi.
Conclusions: We describe a patient with SCA2 who presented with focal dystonia of the right upper extremity. Subtle cerebellar signs as well as the family history became especially important given the absence of predominant gait ataxia. Our case emphasizes that focal dystonia is not only a feature of SCA2, but can also rarely be the presenting sign as well as the most prominent feature during the disease course.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
