Sarah J Nagle, Nirav N Shah, Alex Ganetsky, Daniel J Landsburg, Sunita D Nasta, Anthony Mato, Stephen J Schuster, Ran Reshef, Donald E Tsai, Jakub Svoboda
{"title":"Long-term outcomes of rituximab, temozolomide and high-dose methotrexate without consolidation therapy for lymphoma involving the CNS.","authors":"Sarah J Nagle, Nirav N Shah, Alex Ganetsky, Daniel J Landsburg, Sunita D Nasta, Anthony Mato, Stephen J Schuster, Ran Reshef, Donald E Tsai, Jakub Svoboda","doi":"10.2217/ijh-2017-0020","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>To describe the long-term outcomes of patients with lymphoma in the CNS treated with rituximab, temozolomide and high-dose methotrexate without consolidation therapy.</p><p><strong>Patients & methods: </strong>A retrospective cohort study of 46 consecutive patients with primary CNS lymphoma (PCNSL, 27 patients) or secondary CNS involvement of diffuse large B-cell lymphoma (DLBCL, 19 patients) who were treated with rituximab on day 1 in combination with high-dose methotrexate (days 1 and 15) and temozolomide (days 1-5) in 28-day cycles without further consolidation.</p><p><strong>Results: </strong>Median follow-up was 21.2 months. Patients received a median of five cycles (range 1-15). Median overall survival (OS) was 26 months and median progression-free survival was 8.6 months. At 3 years, 37% of patients were alive and without evidence of disease. The patients with PCNSL had a significantly higher response rates (ORR 81 vs 47%; p = 0.015) and longer median OS (55.3 vs 4.8 months; p < 0.01) than those with secondary CNS DLBCL. Toxicities were mild and manageable.</p><p><strong>Conclusion: </strong>The rituximab, temozolomide and methotrexate regimen is an effective therapy for patients with PCNSL without the toxicities typically associated with consolidation therapy.</p>","PeriodicalId":14166,"journal":{"name":"International Journal of Hematologic Oncology","volume":"6 4","pages":"113-121"},"PeriodicalIF":0.0000,"publicationDate":"2017-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2217/ijh-2017-0020","citationCount":"14","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Hematologic Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2217/ijh-2017-0020","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/1/26 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 14
Abstract
Aim: To describe the long-term outcomes of patients with lymphoma in the CNS treated with rituximab, temozolomide and high-dose methotrexate without consolidation therapy.
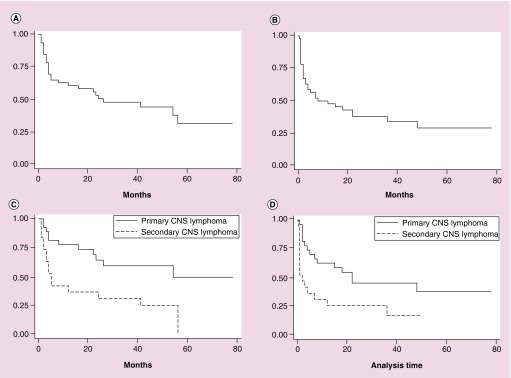
Patients & methods: A retrospective cohort study of 46 consecutive patients with primary CNS lymphoma (PCNSL, 27 patients) or secondary CNS involvement of diffuse large B-cell lymphoma (DLBCL, 19 patients) who were treated with rituximab on day 1 in combination with high-dose methotrexate (days 1 and 15) and temozolomide (days 1-5) in 28-day cycles without further consolidation.
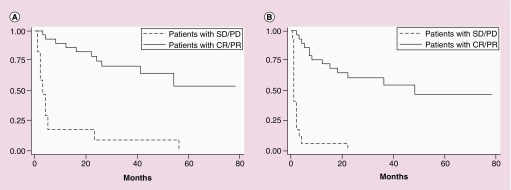
Results: Median follow-up was 21.2 months. Patients received a median of five cycles (range 1-15). Median overall survival (OS) was 26 months and median progression-free survival was 8.6 months. At 3 years, 37% of patients were alive and without evidence of disease. The patients with PCNSL had a significantly higher response rates (ORR 81 vs 47%; p = 0.015) and longer median OS (55.3 vs 4.8 months; p < 0.01) than those with secondary CNS DLBCL. Toxicities were mild and manageable.
Conclusion: The rituximab, temozolomide and methotrexate regimen is an effective therapy for patients with PCNSL without the toxicities typically associated with consolidation therapy.
期刊介绍:
International Journal of Hematologic Oncology welcomes unsolicited article proposals. Email us today to discuss the suitability of your research and our options for authors, including Accelerated Publication. Find out more about publishing open access with us here.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
