Lindsay A Taylor, Michael J Vitto, Michael Joyce, Jordan Tozer, David P Evans
{"title":"Ultrasound-guided thoracostomy site identification in healthy volunteers.","authors":"Lindsay A Taylor, Michael J Vitto, Michael Joyce, Jordan Tozer, David P Evans","doi":"10.1186/s13089-018-0108-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Traditional landmark thoracostomy technique has a known complication rate up to 30%. The goal of this study is to determine whether novice providers could more accurately identify the appropriate intercostal site for thoracostomy by ultrasound guidance.</p><p><strong>Methods: </strong>33 emergency medicine residents and medical students volunteered to participate in this study during routine thoracostomy tube education. A healthy volunteer was used as the standardized patient for this study. An experienced physician sonographer used ultrasound to locate a site at mid-axillary line between ribs 4 and 5 and marked the site with invisible ink that can only be revealed with a commercially available UV LED light. Participants were asked to identify the thoracostomy site by placing an opaque marker where they would make their incision. The distance from the correct insertion site was measured in rib spaces. The participants were then given a brief hands-on training session using ultrasound to identify the diaphragm and count rib spaces. The participants were then asked to use ultrasound to identify the proper thoracostomy site and mark it with an opaque marker. The distance from the proper insertion site was measured and recorded in rib spaces.</p><p><strong>Results: </strong>The participants correctly identified the pre-determined intercostal space using palpation 48% (16/33) of the time, versus the ultrasound group who identified the proper intercostal space 91% (30/33) of the time. On average, the traditional technique was placed 0.88 rib spaces away (95 CI 0.43-1.03), while the ultrasound-guided technique was placed 0.09 rib spaces away (95 CI 0.0-0.19) [P = 0.003].</p><p><strong>Conclusions: </strong>The ability to accurately locate the correct intercostal space for thoracostomy incision was improved under ultrasound guidance. Further studies are warranted to determine if this ultrasound-guided technique will decrease complications with chest tube insertion and improve patient outcomes.</p>","PeriodicalId":46598,"journal":{"name":"Critical Ultrasound Journal","volume":"10 1","pages":"28"},"PeriodicalIF":3.6000,"publicationDate":"2018-10-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13089-018-0108-1","citationCount":"9","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-018-0108-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 9
Abstract
Background: Traditional landmark thoracostomy technique has a known complication rate up to 30%. The goal of this study is to determine whether novice providers could more accurately identify the appropriate intercostal site for thoracostomy by ultrasound guidance.
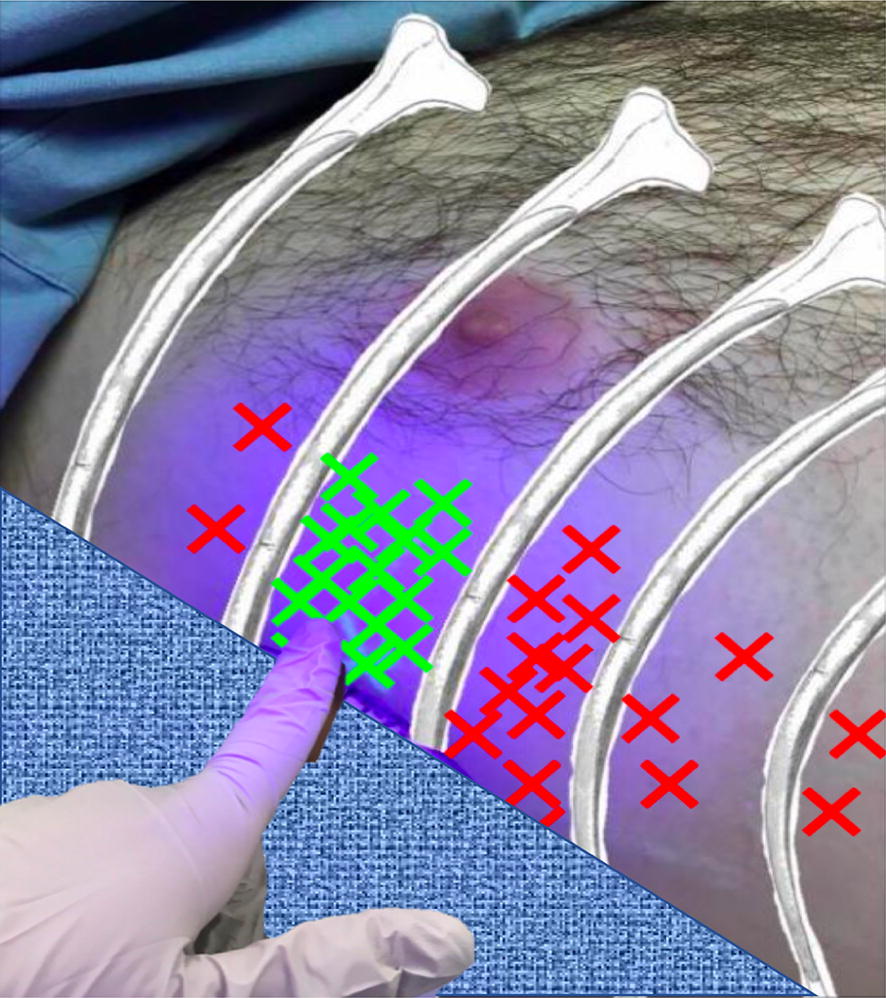
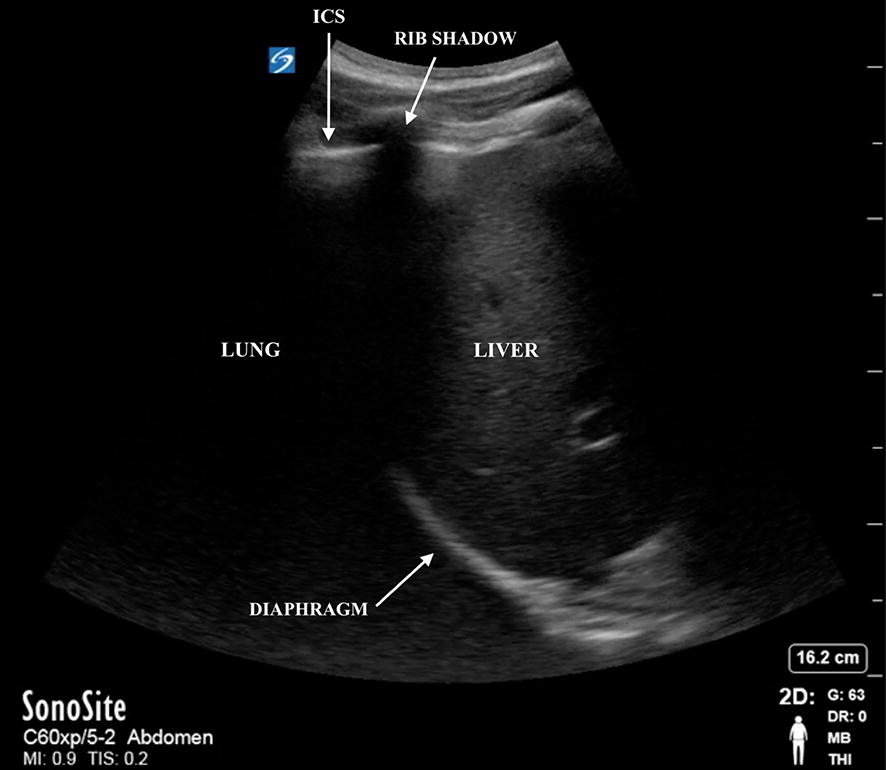
Methods: 33 emergency medicine residents and medical students volunteered to participate in this study during routine thoracostomy tube education. A healthy volunteer was used as the standardized patient for this study. An experienced physician sonographer used ultrasound to locate a site at mid-axillary line between ribs 4 and 5 and marked the site with invisible ink that can only be revealed with a commercially available UV LED light. Participants were asked to identify the thoracostomy site by placing an opaque marker where they would make their incision. The distance from the correct insertion site was measured in rib spaces. The participants were then given a brief hands-on training session using ultrasound to identify the diaphragm and count rib spaces. The participants were then asked to use ultrasound to identify the proper thoracostomy site and mark it with an opaque marker. The distance from the proper insertion site was measured and recorded in rib spaces.
Results: The participants correctly identified the pre-determined intercostal space using palpation 48% (16/33) of the time, versus the ultrasound group who identified the proper intercostal space 91% (30/33) of the time. On average, the traditional technique was placed 0.88 rib spaces away (95 CI 0.43-1.03), while the ultrasound-guided technique was placed 0.09 rib spaces away (95 CI 0.0-0.19) [P = 0.003].
Conclusions: The ability to accurately locate the correct intercostal space for thoracostomy incision was improved under ultrasound guidance. Further studies are warranted to determine if this ultrasound-guided technique will decrease complications with chest tube insertion and improve patient outcomes.
背景:传统的地标性开胸术已知并发症发生率高达30%。本研究的目的是确定新手医生是否可以通过超声引导更准确地确定合适的肋间切口。方法:33名急诊住院医师和医学生在常规开胸插管教育过程中自愿参与本研究。一名健康志愿者作为本研究的标准化患者。一位经验丰富的超声医师使用超声波在第4和第5肋骨之间的腋窝中线定位一个部位,并用隐形墨水标记该部位,这种墨水只能用市售的UV LED灯显示。参与者被要求通过在他们将要切开的地方放置一个不透明的标记来识别开胸部位。在肋骨间隙测量与正确插入位置的距离。然后,参与者接受了一个简短的实践训练课程,使用超声波来识别膈肌和计算肋骨间隙。然后要求参与者使用超声波识别正确的开胸部位,并用不透明的标记进行标记。在肋骨间隙测量并记录与适当插入位置的距离。结果:参与者通过触诊正确识别预先确定的肋间隙的时间为48%(16/33),而超声组识别正确的肋间隙的时间为91%(30/33)。传统技术的平均间距为0.88肋位(95 CI 0.43-1.03),超声引导技术的平均间距为0.09肋位(95 CI 0.0-0.19) [P = 0.003]。结论:超声引导下提高了开胸手术切口正确定位肋间隙的能力。需要进一步的研究来确定这种超声引导技术是否会减少胸管插入的并发症并改善患者的预后。




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
