{"title":"Empagliflozin and Cardio-renal Outcomes in Patients with Type 2 Diabetes and Cardiovascular Disease - Implications for Clinical Practice.","authors":"David H Fitchett","doi":"10.17925/EE.2018.14.2.40","DOIUrl":null,"url":null,"abstract":"<p><p>In patients with type 2 diabetes (T2D), the excretion of glucose by the kidney with sodium-glucose cotransporter 2 (SGLT2) inhibitors lowers glycosylated haemoglobin (HbA1c) levels, decreases body weight and visceral adiposity, as well as improving cardio-renal haemodynamics. Currently, four SGLT2 inhibitors are approved in the US and Europe to improve glycaemic control - empagliflozin, dapagliflozin, canagliflozin, and ertuglifozin. Recently, the SGLT2 inhibitor empagliflozin was approved by the FDA for the reduction of cardiovascular (CV) death in adults with T2D and CV disease (CVD). This approval was based on the findings of the Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG OUTCOME) study, which was the first study to show a significant reduction of a primary CV endpoint with a glucose-lowering agent. In this study, the primary outcome (CV mortality, non-fatal myocardial infarction [MI] and non-fatal stroke) was reduced by empagliflozin (10.5%; 490/4,687) compared with placebo (12.1%; 282/2,333); hazard ratio (HR), 0.86 (95% confidence interval [CI]: 0.74, 0.99). The primary outcome was driven by a large reduction of CV mortality (relative risk reduction [RRR], 38%). Empagliflozin also reduced all-cause mortality (RRR, 32%). Furthermore, empagliflozin reduced the adjudicated outcome of heart failure (HF) hospitalisation by 35% (HR, 0.65; 95% CI: 0.50, 0.85). Other non-adjudicated measures of HF outcomes were similarly reduced including investigator reported HF, the introduction of loop diuretics and death from HF. In the analysis of renal outcomes, incident or worsening nephropathy was reduced for empagliflozin (12.7%) compared with placebo (18.8%); HR, 0.61 (95% CI: 0.53, 0.70). Empagliflozin significantly reduced the risk of progression to macroalbuminuria (38%) and doubling of creatinine (44%), as well as the need of starting renal-replacement therapy (55%). The benefits of empagliflozin for the reduction of CV death, all-cause death and hospitalisation for HF were observed across a range of baseline subgroups such as HbA1c level and renal function (down to estimated glomerular filtration rate [eGFR] 30 ml/min/1.73 m<sup>2</sup>). The rapid reduction of HF outcomes with empagliflozin is observed across the spectrum of CVD and HF risk and represents a therapeutic advance in the prevention and perhaps also in the treatment of HF, an often poorly recognised complication of T2D. This review discusses the EMPA-REG OUTCOME study and the implications for treating patients with T2D and CVD.</p>","PeriodicalId":38860,"journal":{"name":"European Endocrinology","volume":"14 2","pages":"40-49"},"PeriodicalIF":0.0000,"publicationDate":"2018-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4a/5f/euendo-14-40.PMC6182918.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17925/EE.2018.14.2.40","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/9/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
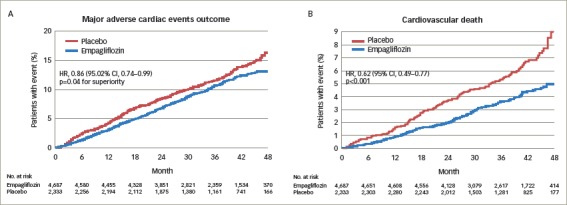
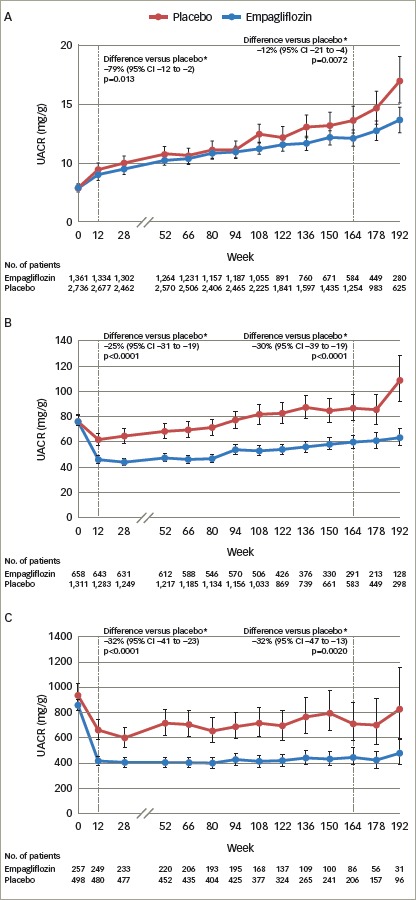
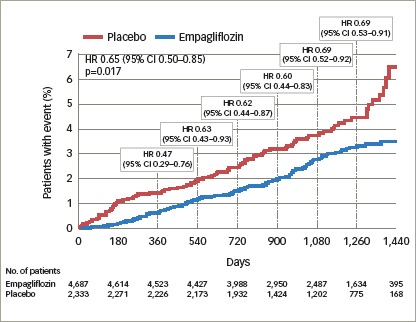
In patients with type 2 diabetes (T2D), the excretion of glucose by the kidney with sodium-glucose cotransporter 2 (SGLT2) inhibitors lowers glycosylated haemoglobin (HbA1c) levels, decreases body weight and visceral adiposity, as well as improving cardio-renal haemodynamics. Currently, four SGLT2 inhibitors are approved in the US and Europe to improve glycaemic control - empagliflozin, dapagliflozin, canagliflozin, and ertuglifozin. Recently, the SGLT2 inhibitor empagliflozin was approved by the FDA for the reduction of cardiovascular (CV) death in adults with T2D and CV disease (CVD). This approval was based on the findings of the Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes (EMPA-REG OUTCOME) study, which was the first study to show a significant reduction of a primary CV endpoint with a glucose-lowering agent. In this study, the primary outcome (CV mortality, non-fatal myocardial infarction [MI] and non-fatal stroke) was reduced by empagliflozin (10.5%; 490/4,687) compared with placebo (12.1%; 282/2,333); hazard ratio (HR), 0.86 (95% confidence interval [CI]: 0.74, 0.99). The primary outcome was driven by a large reduction of CV mortality (relative risk reduction [RRR], 38%). Empagliflozin also reduced all-cause mortality (RRR, 32%). Furthermore, empagliflozin reduced the adjudicated outcome of heart failure (HF) hospitalisation by 35% (HR, 0.65; 95% CI: 0.50, 0.85). Other non-adjudicated measures of HF outcomes were similarly reduced including investigator reported HF, the introduction of loop diuretics and death from HF. In the analysis of renal outcomes, incident or worsening nephropathy was reduced for empagliflozin (12.7%) compared with placebo (18.8%); HR, 0.61 (95% CI: 0.53, 0.70). Empagliflozin significantly reduced the risk of progression to macroalbuminuria (38%) and doubling of creatinine (44%), as well as the need of starting renal-replacement therapy (55%). The benefits of empagliflozin for the reduction of CV death, all-cause death and hospitalisation for HF were observed across a range of baseline subgroups such as HbA1c level and renal function (down to estimated glomerular filtration rate [eGFR] 30 ml/min/1.73 m2). The rapid reduction of HF outcomes with empagliflozin is observed across the spectrum of CVD and HF risk and represents a therapeutic advance in the prevention and perhaps also in the treatment of HF, an often poorly recognised complication of T2D. This review discusses the EMPA-REG OUTCOME study and the implications for treating patients with T2D and CVD.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
