Markus Meier, Wolfram Johannes Jabs, Maria Guthmann, Gesa Geppert, Ali Aydin, Martin Nitschke
{"title":"Sonographic Venous Velocity Index Identifies Patients with Chronic Kidney Disease and Severe Diastolic Dysfunction.","authors":"Markus Meier, Wolfram Johannes Jabs, Maria Guthmann, Gesa Geppert, Ali Aydin, Martin Nitschke","doi":"10.1055/a-0684-9483","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Diagnosing cardiorenal syndrome (CRS) in patients with chronic kidney disease (CKD) continues to remain challenging in outpatient practice. In this study, we investigate whether a newly developed venous velocity ultrasound index (VVI) can differentiate between patients with CRS and patients with CKD of other cause or normal renal function (NRF).</p><p><strong>Methods: </strong>Patients with CRS (n <b>=</b> 30), CKD (n=30), and NRF (n=30) were included in the study. For each patient, duplex ultrasound scans of intrarenal segmental veins were retrospectively analyzed. The VVI was calculated from the renal venous doppler curve as the ratio of the maximal positive venous velocity to the maximal negative venous velocity. Patients with CRS were compared to age-matched controls with NRF and to GFR-matched controls with CKD.</p><p><strong>Results: </strong>The GFRs of patients with CRS and those with CKD were comparable (26.4±5 and 25.6±7 ml/min/m2), as was the age in patients with CRS and NRF (6 ±12 years and 68±16 years, respectively). There was no significant difference in ejection fraction between patients with CRS and those with CKD (44.2±6.2% vs. 47.4 ±7.2), but there was a significant decrease compared to those with NRF (52.6 ±5.1, p<0.01). The VVI was significantly higher in the CRS group (0.81± 0.18) compared to the CKD group (0.18± 0.17, p<0.01) or NRF group (0.22± 0.20, p<0.01). The positive predictability of CRS was 96.4% in patients with VVI values of >0.6.</p><p><strong>Conclusion: </strong>The newly developed VVI was useful in successfully predicting severe diastolic dysfunction (CRS) in patients with severe kidney injury in outpatient care.</p>","PeriodicalId":44852,"journal":{"name":"Ultrasound International Open","volume":"4 4","pages":"E142-E148"},"PeriodicalIF":1.6000,"publicationDate":"2018-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1055/a-0684-9483","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound International Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/a-0684-9483","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2018/10/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 1
Abstract
Objective: Diagnosing cardiorenal syndrome (CRS) in patients with chronic kidney disease (CKD) continues to remain challenging in outpatient practice. In this study, we investigate whether a newly developed venous velocity ultrasound index (VVI) can differentiate between patients with CRS and patients with CKD of other cause or normal renal function (NRF).
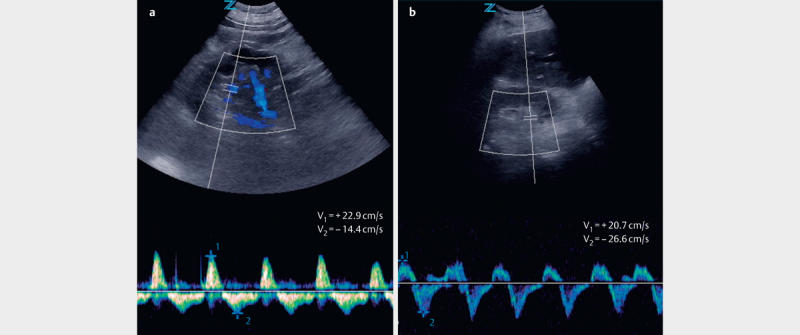
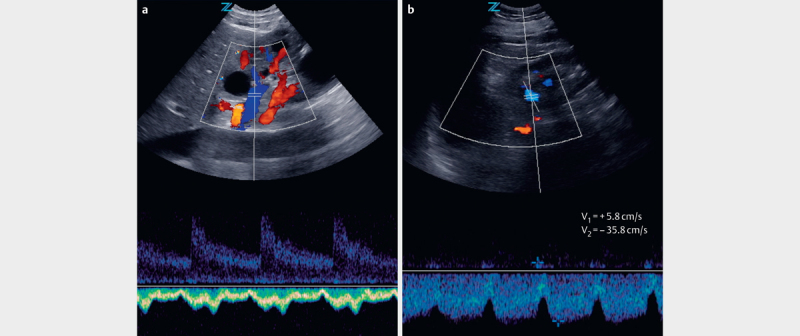
Methods: Patients with CRS (n = 30), CKD (n=30), and NRF (n=30) were included in the study. For each patient, duplex ultrasound scans of intrarenal segmental veins were retrospectively analyzed. The VVI was calculated from the renal venous doppler curve as the ratio of the maximal positive venous velocity to the maximal negative venous velocity. Patients with CRS were compared to age-matched controls with NRF and to GFR-matched controls with CKD.
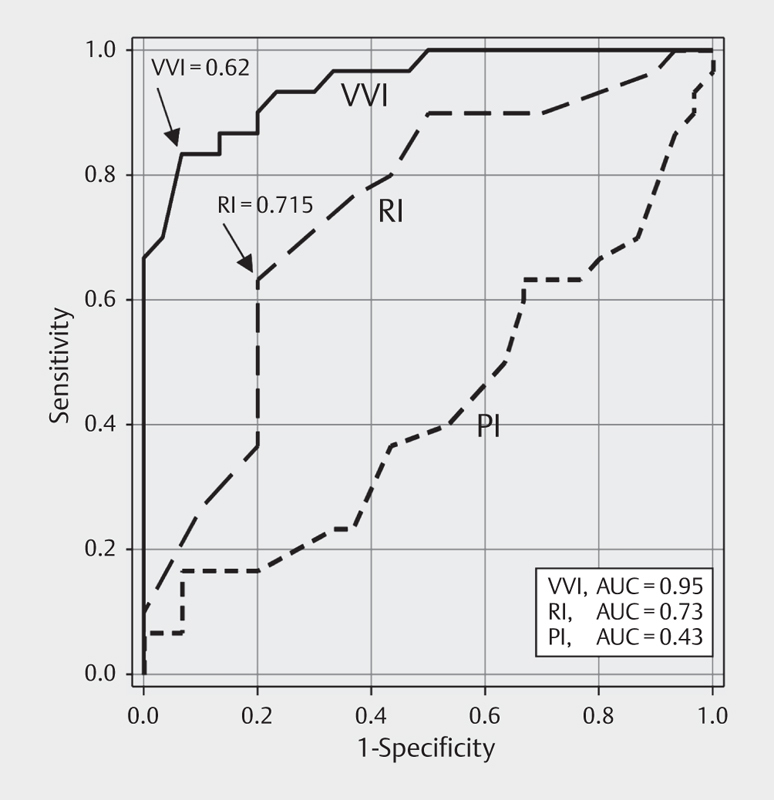
Results: The GFRs of patients with CRS and those with CKD were comparable (26.4±5 and 25.6±7 ml/min/m2), as was the age in patients with CRS and NRF (6 ±12 years and 68±16 years, respectively). There was no significant difference in ejection fraction between patients with CRS and those with CKD (44.2±6.2% vs. 47.4 ±7.2), but there was a significant decrease compared to those with NRF (52.6 ±5.1, p<0.01). The VVI was significantly higher in the CRS group (0.81± 0.18) compared to the CKD group (0.18± 0.17, p<0.01) or NRF group (0.22± 0.20, p<0.01). The positive predictability of CRS was 96.4% in patients with VVI values of >0.6.
Conclusion: The newly developed VVI was useful in successfully predicting severe diastolic dysfunction (CRS) in patients with severe kidney injury in outpatient care.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
