A V Trailin, T N Nykonenko, T I Ostapenko, S R Vildanov, O S Nykonenko
{"title":"Significance of the Pathologic Findings in Implantation Biopsies for Kidney Allografts Survival.","authors":"A V Trailin, T N Nykonenko, T I Ostapenko, S R Vildanov, O S Nykonenko","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is no consistent association between individual histological lesions and composite scores in donor kidney biopsy and transplant outcomes.</p><p><strong>Objective: </strong>To evaluate which acute or chronic individual histological lesions and composite scores in donor kidney were associated with graft survival in the recipient.</p><p><strong>Methods: </strong>We investigated the association of individual histological lesions and 8 composite scoring systems in implantation biopsies of cadaveric (n=101) and living (n=29) kidneys with 5-year death-censored graft survival.</p><p><strong>Results: </strong>We found a high frequency of chronic lesions in donor kidneys, mostly associated with arteriosclerosis, and less dependent from donor age. Acute, chronic, and total Banff scores for post-transplant biopsies, chronic and total Banff scores for pre-implant biopsies, donor damage score and chronic damage score predicted death-censored graft loss. However, only chronic and total Banff-scores had significant effects in multivariate model. Chronic pre-implant and total post-transplant Banff scores demonstrated the highest area under the curve (AUC) of 0.722 and 0.717, respectively. Among individual lesions, glomerulosclerosis ≥20%, interstitial inflammation >0, arteriosclerosis =3, arteriolar hyalinosis >0, and interstitial fibrosis >0, assessed with Banff-grading criteria, were associated with lower allograft survival. We created the Donor Kidney Damage Index (DKDI), by summing regression coefficients for these lesions, which yielded the AUC of 0.747. When combined with retransplantation, cold ischemia time and acute rejection, DKDI, chronic pre-implant and total post-transplant Banff scores further improved their predictive accuracy, yielding AUCs of 0.842, 0.807, and 0.802, respectively.</p><p><strong>Conclusion: </strong>DKDI, chronic pre-implant and total post-transplant Banff scores alone and combined with clinical variables may facilitate decision making in post-transplant period.</p>","PeriodicalId":14242,"journal":{"name":"International Journal of Organ Transplantation Medicine","volume":"10 1","pages":"15-29"},"PeriodicalIF":0.2000,"publicationDate":"2019-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6416998/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Organ Transplantation Medicine","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/2/1 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: There is no consistent association between individual histological lesions and composite scores in donor kidney biopsy and transplant outcomes.
Objective: To evaluate which acute or chronic individual histological lesions and composite scores in donor kidney were associated with graft survival in the recipient.
Methods: We investigated the association of individual histological lesions and 8 composite scoring systems in implantation biopsies of cadaveric (n=101) and living (n=29) kidneys with 5-year death-censored graft survival.
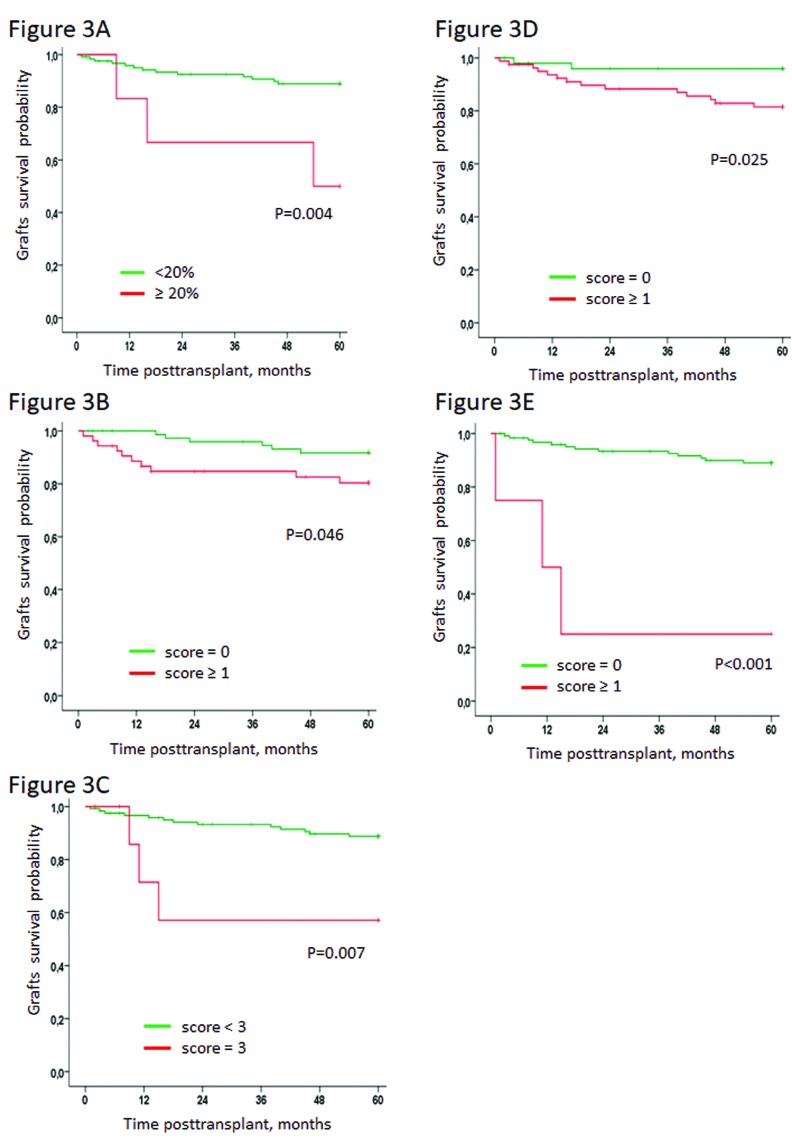
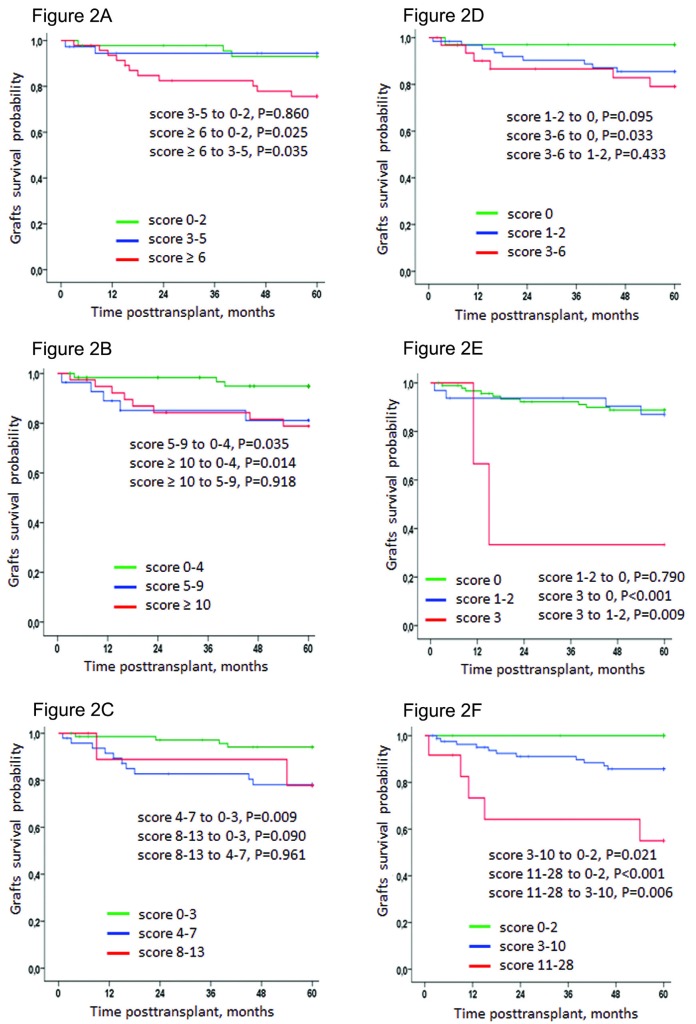
Results: We found a high frequency of chronic lesions in donor kidneys, mostly associated with arteriosclerosis, and less dependent from donor age. Acute, chronic, and total Banff scores for post-transplant biopsies, chronic and total Banff scores for pre-implant biopsies, donor damage score and chronic damage score predicted death-censored graft loss. However, only chronic and total Banff-scores had significant effects in multivariate model. Chronic pre-implant and total post-transplant Banff scores demonstrated the highest area under the curve (AUC) of 0.722 and 0.717, respectively. Among individual lesions, glomerulosclerosis ≥20%, interstitial inflammation >0, arteriosclerosis =3, arteriolar hyalinosis >0, and interstitial fibrosis >0, assessed with Banff-grading criteria, were associated with lower allograft survival. We created the Donor Kidney Damage Index (DKDI), by summing regression coefficients for these lesions, which yielded the AUC of 0.747. When combined with retransplantation, cold ischemia time and acute rejection, DKDI, chronic pre-implant and total post-transplant Banff scores further improved their predictive accuracy, yielding AUCs of 0.842, 0.807, and 0.802, respectively.
Conclusion: DKDI, chronic pre-implant and total post-transplant Banff scores alone and combined with clinical variables may facilitate decision making in post-transplant period.
期刊介绍:
The International Journal of Organ Transplantation Medicine (IJOTM) is a quarterly peer-reviewed English-language journal that publishes high-quality basic sciences and clinical research on transplantation. The scope of the journal includes organ and tissue donation, procurement and preservation; surgical techniques, innovations, and novelties in all aspects of transplantation; genomics and immunobiology; immunosuppressive drugs and pharmacology relevant to transplantation; graft survival and prevention of graft dysfunction and failure; clinical trials and population analyses in the field of transplantation; transplant complications; cell and tissue transplantation; infection; post-transplant malignancies; sociological and ethical issues and xenotransplantation.
 分享
分享



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
