Vascular Reconstructions in Living Unrelated Kidney Transplant Using Donor Ovarian Vein and Recipient Inferior Epigastric Artery with Simultaneous Enucleation of a Complex Cyst.
Giuseppe Serena, Javier Gonzalez, Giselle Guerra, Mohamed Ammar Al Nuss, Maykel Valdes, Gaetano Ciancio
{"title":"Vascular Reconstructions in Living Unrelated Kidney Transplant Using Donor Ovarian Vein and Recipient Inferior Epigastric Artery with Simultaneous Enucleation of a Complex Cyst.","authors":"Giuseppe Serena, Javier Gonzalez, Giselle Guerra, Mohamed Ammar Al Nuss, Maykel Valdes, Gaetano Ciancio","doi":"10.1155/2019/3272080","DOIUrl":null,"url":null,"abstract":"<p><p>Increasing the organ donor pool and solving the recipient demands continue to be one of the challenges in transplantation. We report our experience in transplanting a living donor kidney requiring complex vascular reconstructions and an enucleation of complex cyst. A 57-year-old male patient underwent a living unrelated kidney transplant. The living donor kidney was procured through a laparoscopic hand-assisted right donor nephrectomy. After vascular stapling, the kidney had a short upper pole arterial branch, a short renal vein (3 mm), and a complex upper pole cyst. The renal vein was elongated using the donor ovarian vein and the short upper pole artery was extended using the recipient inferior epigastric artery and anastomosed to the main renal artery. The renal allograft vessels were anastomosed end-to-side to the external iliac vessels. The complex cyst was removed performing an enucleation with a rim of normal tissue and reconstruction of the calyceal system. This case represents three different surgical reconstructions in order to make the organ available for transplantation. In some circumstances, complex vascular reconstruction of living donor kidney with removal of complex cyst represents a strategy to expand the donor pool.</p>","PeriodicalId":30327,"journal":{"name":"Case Reports in Transplantation","volume":"2019 ","pages":"3272080"},"PeriodicalIF":0.0000,"publicationDate":"2019-03-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2019/3272080","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Transplantation","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/3272080","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
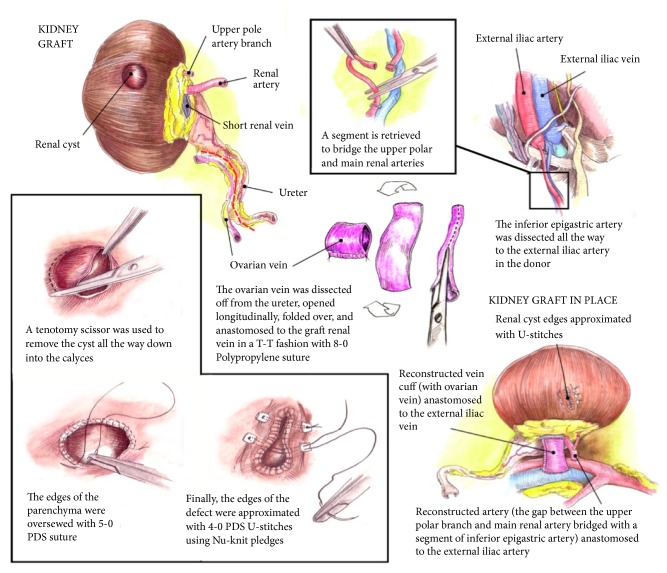
Increasing the organ donor pool and solving the recipient demands continue to be one of the challenges in transplantation. We report our experience in transplanting a living donor kidney requiring complex vascular reconstructions and an enucleation of complex cyst. A 57-year-old male patient underwent a living unrelated kidney transplant. The living donor kidney was procured through a laparoscopic hand-assisted right donor nephrectomy. After vascular stapling, the kidney had a short upper pole arterial branch, a short renal vein (3 mm), and a complex upper pole cyst. The renal vein was elongated using the donor ovarian vein and the short upper pole artery was extended using the recipient inferior epigastric artery and anastomosed to the main renal artery. The renal allograft vessels were anastomosed end-to-side to the external iliac vessels. The complex cyst was removed performing an enucleation with a rim of normal tissue and reconstruction of the calyceal system. This case represents three different surgical reconstructions in order to make the organ available for transplantation. In some circumstances, complex vascular reconstruction of living donor kidney with removal of complex cyst represents a strategy to expand the donor pool.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
