Delayed Antiretroviral Therapy (ART) Initiation among Hospitalized Adults in a Resource-Limited Settings: A Challenge to the Global Target of ART for 90% of HIV-Infected Individuals.
Prossie Merab Ingabire, Fred Semitala, Moses R Kamya, Damalie Nakanjako
{"title":"Delayed Antiretroviral Therapy (ART) Initiation among Hospitalized Adults in a Resource-Limited Settings: A Challenge to the Global Target of ART for 90% of HIV-Infected Individuals.","authors":"Prossie Merab Ingabire, Fred Semitala, Moses R Kamya, Damalie Nakanjako","doi":"10.1155/2019/1832152","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Combination antiretroviral therapy (cART) initiation in hospital settings, where individuals often present with undiagnosed, untreated, advanced HIV disease, is not well understood.</p><p><strong>Methods: </strong>A cross-sectional study was conducted to determine a period prevalence of cART initiation within two weeks of eligibility, as determined at hospitalization. Using a pretested and precoded data extraction tool, data on cART initiation status and reason for not initiating cART was collected. Phone calls were made to patients that had left the hospital by the end of the two-week period. Delayed cART initiation was defined as failure to initiate cART within two weeks. Sociodemographic characteristics, WHO clinical stage, CD4 count, cART initiation status, and reasons for delayed cART initiation were extracted and analyzed.</p><p><strong>Results: </strong>Overall, 386 HIV-infected adults were enrolled, of whom 289/386 (74.9%) had delayed cART initiation, 77/386 (19.9%) initiated cART, and 20/386 (5.2%) were lost-to-follow-up, within two weeks of cART eligibility. Of 289 with delayed ART initiation, 94 (32.5%) died within two weeks of cART eligibility. Patients with a CD4 cell count≥ 50 cells/<i>μ</i>l and who resided in ≥8 kilometers from the hospital were more likely to have delayed cART initiation [adjusted odds ratio (AOR) 2.34, 95% CI: 1.33-4.10, p value 0.003; and AOR 1.92, 95% CI: 1.09-3.40, p value 0.025; respectively].</p><p><strong>Conclusion: </strong>Up to 75% of hospitalized HIV-infected, cART-naïve, cART-eligible patients did not initiate cART and had a 33% pre-ART mortality rate within two weeks of eligibility for cART. Hospital based strategies to hasten cART initiation during hospitalization and electronic patient tracking systems could promote active linkage to HIV treatment programs, to prevent HIV/AIDS-associated mortality in resource-limited settings.</p>","PeriodicalId":46303,"journal":{"name":"AIDS Research and Treatment","volume":"2019 ","pages":"1832152"},"PeriodicalIF":1.8000,"publicationDate":"2019-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6463639/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AIDS Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2019/1832152","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Combination antiretroviral therapy (cART) initiation in hospital settings, where individuals often present with undiagnosed, untreated, advanced HIV disease, is not well understood.
Methods: A cross-sectional study was conducted to determine a period prevalence of cART initiation within two weeks of eligibility, as determined at hospitalization. Using a pretested and precoded data extraction tool, data on cART initiation status and reason for not initiating cART was collected. Phone calls were made to patients that had left the hospital by the end of the two-week period. Delayed cART initiation was defined as failure to initiate cART within two weeks. Sociodemographic characteristics, WHO clinical stage, CD4 count, cART initiation status, and reasons for delayed cART initiation were extracted and analyzed.
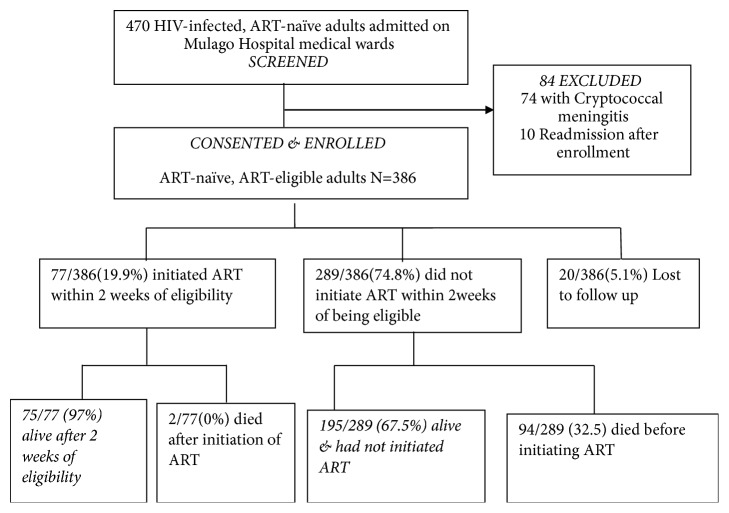
Results: Overall, 386 HIV-infected adults were enrolled, of whom 289/386 (74.9%) had delayed cART initiation, 77/386 (19.9%) initiated cART, and 20/386 (5.2%) were lost-to-follow-up, within two weeks of cART eligibility. Of 289 with delayed ART initiation, 94 (32.5%) died within two weeks of cART eligibility. Patients with a CD4 cell count≥ 50 cells/μl and who resided in ≥8 kilometers from the hospital were more likely to have delayed cART initiation [adjusted odds ratio (AOR) 2.34, 95% CI: 1.33-4.10, p value 0.003; and AOR 1.92, 95% CI: 1.09-3.40, p value 0.025; respectively].
Conclusion: Up to 75% of hospitalized HIV-infected, cART-naïve, cART-eligible patients did not initiate cART and had a 33% pre-ART mortality rate within two weeks of eligibility for cART. Hospital based strategies to hasten cART initiation during hospitalization and electronic patient tracking systems could promote active linkage to HIV treatment programs, to prevent HIV/AIDS-associated mortality in resource-limited settings.
期刊介绍:
AIDS Research and Treatment is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies focused on all aspects of HIV and AIDS, from the molecular basis of disease to translational and clinical research. In addition, articles relating to prevention, education, and behavior change will be considered



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
