Sreedhar Adapa, Venu Madhav Konala, Srikanth Naramala, Cynthia C Nast
{"title":"Multiple morphological phenotypes of monoclonal immunoglobulin disease on renal biopsy: Significance of treatment.","authors":"Sreedhar Adapa, Venu Madhav Konala, Srikanth Naramala, Cynthia C Nast","doi":"10.5414/CNCS110052","DOIUrl":null,"url":null,"abstract":"<p><p>Plasma cell dyscrasias frequently involve the kidney causing renal dysfunction. Multiple morphologic manifestations of κ light chain disease occurring simultaneously in the same kidney biopsy are uncommon and suggest local microenvironment effects in addition to structural properties of the light chain. A 61-year-old female presented with new onset renal failure and proteinuria. Serological workup revealed monoclonal gammopathy with elevated κ : λ ratio of 1,371. Renal biopsy revealed several paraprotein manifestations including κ light chain deposition disease, monoclonal fibrillary glomerulonephritis, cryocrystalglobulenemia and fibrillar/microtubular cast nephropathy. There was also incidental leukocyte chemotactic factor 2 amyloidosis (ALECT 2), negative for κ light chain and confirmed by immunohistochemistry (IHC). Bone marrow biopsy revealed 10 - 20% κ restricted plasma cells. The patient received 10 cycles of CyBorD (cyclophosphamide, bortezomib, and dexamethasone) chemotherapy. Renal function improved with decreased κ : λ ratio. Repeat bone marrow biopsy showed no evidence of abnormal plasma cells by IHC. The renal recovery demonstrates there may be response to chemotherapy irrespective of the morphologic manifestations of light chain-related injury. Additionally, if amyloid is not demonstrated to be of light chain origin, other amyloid types should be considered.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"8 ","pages":"17-24"},"PeriodicalIF":0.0000,"publicationDate":"2020-04-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7171697/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110052","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
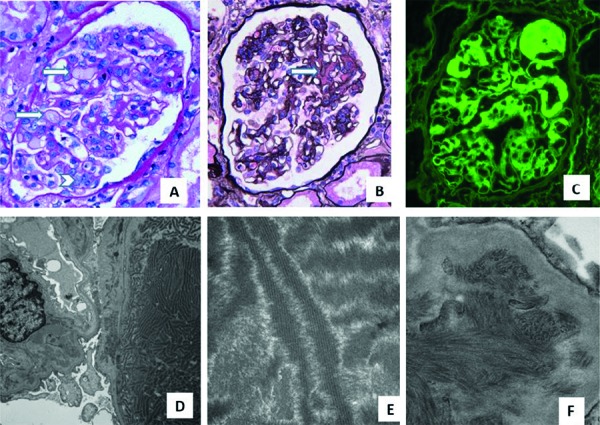
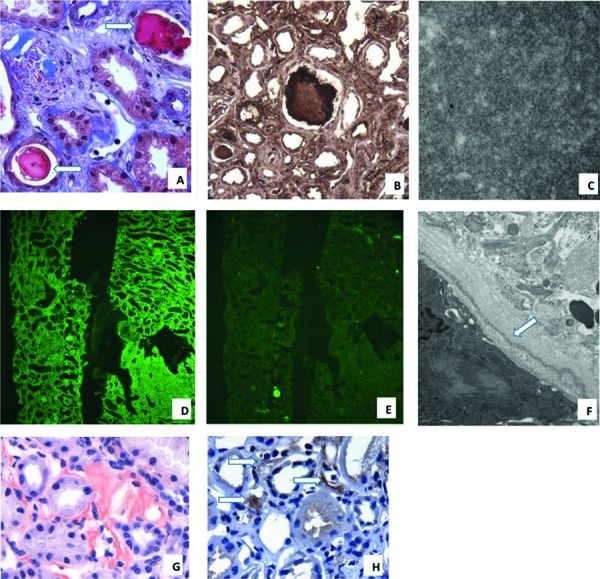
Plasma cell dyscrasias frequently involve the kidney causing renal dysfunction. Multiple morphologic manifestations of κ light chain disease occurring simultaneously in the same kidney biopsy are uncommon and suggest local microenvironment effects in addition to structural properties of the light chain. A 61-year-old female presented with new onset renal failure and proteinuria. Serological workup revealed monoclonal gammopathy with elevated κ : λ ratio of 1,371. Renal biopsy revealed several paraprotein manifestations including κ light chain deposition disease, monoclonal fibrillary glomerulonephritis, cryocrystalglobulenemia and fibrillar/microtubular cast nephropathy. There was also incidental leukocyte chemotactic factor 2 amyloidosis (ALECT 2), negative for κ light chain and confirmed by immunohistochemistry (IHC). Bone marrow biopsy revealed 10 - 20% κ restricted plasma cells. The patient received 10 cycles of CyBorD (cyclophosphamide, bortezomib, and dexamethasone) chemotherapy. Renal function improved with decreased κ : λ ratio. Repeat bone marrow biopsy showed no evidence of abnormal plasma cells by IHC. The renal recovery demonstrates there may be response to chemotherapy irrespective of the morphologic manifestations of light chain-related injury. Additionally, if amyloid is not demonstrated to be of light chain origin, other amyloid types should be considered.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
