Minimally Invasive Parafascicular Surgery (MIPS) for Spontaneous Intracerebral Hemorrhage Compared to Medical Management: A Case Series Comparison for a Single Institution.
Victoria L Phillips, Anil K Roy, Jonathan Ratcliff, Gustavo Pradilla
{"title":"Minimally Invasive Parafascicular Surgery (MIPS) for Spontaneous Intracerebral Hemorrhage Compared to Medical Management: A Case Series Comparison for a Single Institution.","authors":"Victoria L Phillips, Anil K Roy, Jonathan Ratcliff, Gustavo Pradilla","doi":"10.1155/2020/6503038","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We compared the safety and effectiveness of minimally invasive parafascicular surgery (MIPS) as a frontline treatment for spontaneous supratentorial ICH to medical management. <i>Patients</i>. The sample consisted of 17 patients who underwent MIPS from January 2014 to December 2016 and a comparison group of 23 patients who were medically managed from June 2012 to December 2013. All had an International Classification of Disease (ICD) diagnosis of 431 and were treated at Grady Memorial Hospital, an urban, public, safety-net hospital.</p><p><strong>Methods: </strong>The primary endpoint was risk of inpatient mortality. Secondary endpoints were rates of inpatient infection and favorable discharge status, defined as discharge to home or rehabilitation facility. Demographics and pre- and postclinical outcomes were compared using <i>t</i>-tests, the Mann-Whitney test, and chi-squared tests for continuous, ordinal and categorical measures, respectively. Cox proportional hazard models were used to estimate the time to inpatient death. Logistic regression analyses were used to determine treatment effects on secondary outcomes. We also conducted exploratory subgroup analyses which compared MIPS to two medical management subgroups: those who had surgery during their hospitalization and those that did not.</p><p><strong>Results: </strong>Two patients (12%) died in the MIPS group compared to three (12%) in the medical management group. MIPS did not increase the risk of inpatient mortality relative to medical management. Rates of inpatient infection did not differ significantly between the two groups; eight MIPS patients (47%) and 13 medically managed patients (50%) contracted infections. MIPS significantly increased the likelihood of favorable discharge status (odds ratio (OR) 1.77; 95% CI, 1.12-21.9) compared to medical management. No outcome measures were significantly different between MIPS and the medical management subgroup without surgery, while rates of favorable discharge were higher among the MIPS patients compared to the medical management group with surgery.</p><p><strong>Conclusions: </strong>These data suggest that MIPS, as a frontline treatment for spontaneous ICH, versus medical management for spontaneous ICH warrants further investigation.</p>","PeriodicalId":22054,"journal":{"name":"Stroke Research and Treatment","volume":"2020 ","pages":"6503038"},"PeriodicalIF":1.6000,"publicationDate":"2020-06-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7306855/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Stroke Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/6503038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: We compared the safety and effectiveness of minimally invasive parafascicular surgery (MIPS) as a frontline treatment for spontaneous supratentorial ICH to medical management. Patients. The sample consisted of 17 patients who underwent MIPS from January 2014 to December 2016 and a comparison group of 23 patients who were medically managed from June 2012 to December 2013. All had an International Classification of Disease (ICD) diagnosis of 431 and were treated at Grady Memorial Hospital, an urban, public, safety-net hospital.
Methods: The primary endpoint was risk of inpatient mortality. Secondary endpoints were rates of inpatient infection and favorable discharge status, defined as discharge to home or rehabilitation facility. Demographics and pre- and postclinical outcomes were compared using t-tests, the Mann-Whitney test, and chi-squared tests for continuous, ordinal and categorical measures, respectively. Cox proportional hazard models were used to estimate the time to inpatient death. Logistic regression analyses were used to determine treatment effects on secondary outcomes. We also conducted exploratory subgroup analyses which compared MIPS to two medical management subgroups: those who had surgery during their hospitalization and those that did not.
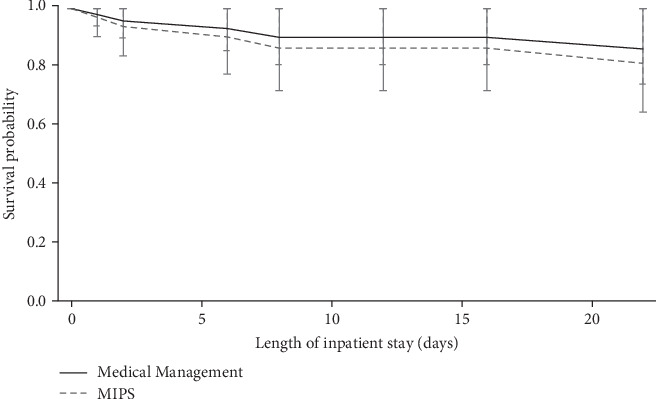
Results: Two patients (12%) died in the MIPS group compared to three (12%) in the medical management group. MIPS did not increase the risk of inpatient mortality relative to medical management. Rates of inpatient infection did not differ significantly between the two groups; eight MIPS patients (47%) and 13 medically managed patients (50%) contracted infections. MIPS significantly increased the likelihood of favorable discharge status (odds ratio (OR) 1.77; 95% CI, 1.12-21.9) compared to medical management. No outcome measures were significantly different between MIPS and the medical management subgroup without surgery, while rates of favorable discharge were higher among the MIPS patients compared to the medical management group with surgery.
Conclusions: These data suggest that MIPS, as a frontline treatment for spontaneous ICH, versus medical management for spontaneous ICH warrants further investigation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
