Heather E Whitson, Alexandra M Hajduk, Xuemei Song, Mary Geda, Sui Tsang, John Brush, Sarwat I Chaudhry
{"title":"Comorbid vision and cognitive impairments in older adults hospitalized for acute myocardial infarction.","authors":"Heather E Whitson, Alexandra M Hajduk, Xuemei Song, Mary Geda, Sui Tsang, John Brush, Sarwat I Chaudhry","doi":"10.1177/2235042X20940493","DOIUrl":null,"url":null,"abstract":"<p><p>Older patients presenting with acute myocardial infarction (AMI) often have comorbidities. Our objective was to examine how outcomes differ by cognitive and vision status in older AMI patients. We use data from a prospective cohort study conducted at 94 hospitals in the United States between January 2013 and October 2016 that enrolled men and women aged ≥75 years with AMI. Cognitive impairment (CI) was defined as telephone interview for cognitive status (TICS) score <27; vision impairment (VI) and activities of daily living (ADLs) were assessed by questionnaire. Of 2988 senior AMI patients, 260 (8.7%) had CI but no VI, 858 (28.7%) had VI but no CI, and 251 (8.4%) had both CI/VI. Patients in the VI/CI group were most likely to exhibit geriatric syndromes. More severe VI was associated with lower (worse) scores on the TICS (<i>β</i> -1.53, 95% confidence interval (CI) -1.87 to -1.18). In adjusted models, compared to participants with neither impairment, participants with VI/CI were more likely to die (hazard ratio 1.61, 95% CI 1.10-2.37) and experience ADL decline (odds ratio 2.11, 95% CI 1.39-3.21) at 180 days. Comorbid CIs and VIs were associated with high rates of death and worsening disability after discharge among seniors hospitalized for AMI. Future research should evaluate protocols to accommodate these impairments during AMI presentations and optimize decision-making and outcomes.</p>","PeriodicalId":92071,"journal":{"name":"Journal of comorbidity","volume":"10 ","pages":"2235042X20940493"},"PeriodicalIF":0.0000,"publicationDate":"2020-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7366400/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of comorbidity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2235042X20940493","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
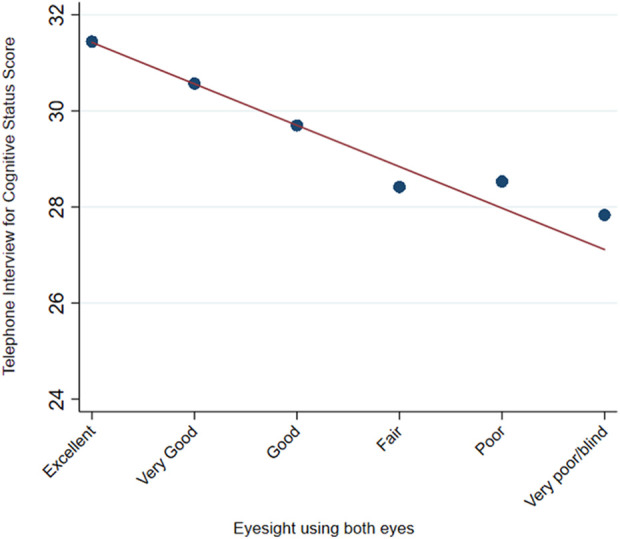
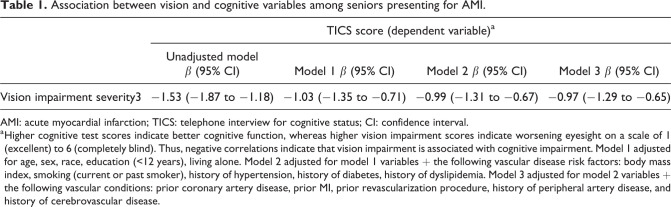
Older patients presenting with acute myocardial infarction (AMI) often have comorbidities. Our objective was to examine how outcomes differ by cognitive and vision status in older AMI patients. We use data from a prospective cohort study conducted at 94 hospitals in the United States between January 2013 and October 2016 that enrolled men and women aged ≥75 years with AMI. Cognitive impairment (CI) was defined as telephone interview for cognitive status (TICS) score <27; vision impairment (VI) and activities of daily living (ADLs) were assessed by questionnaire. Of 2988 senior AMI patients, 260 (8.7%) had CI but no VI, 858 (28.7%) had VI but no CI, and 251 (8.4%) had both CI/VI. Patients in the VI/CI group were most likely to exhibit geriatric syndromes. More severe VI was associated with lower (worse) scores on the TICS (β -1.53, 95% confidence interval (CI) -1.87 to -1.18). In adjusted models, compared to participants with neither impairment, participants with VI/CI were more likely to die (hazard ratio 1.61, 95% CI 1.10-2.37) and experience ADL decline (odds ratio 2.11, 95% CI 1.39-3.21) at 180 days. Comorbid CIs and VIs were associated with high rates of death and worsening disability after discharge among seniors hospitalized for AMI. Future research should evaluate protocols to accommodate these impairments during AMI presentations and optimize decision-making and outcomes.
老年急性心肌梗死(AMI)患者常伴有合并症。我们的目的是研究老年AMI患者的认知和视力状况对预后的影响。我们使用的数据来自2013年1月至2016年10月期间在美国94家医院进行的前瞻性队列研究,纳入了年龄≥75岁的AMI患者。认知障碍(CI)定义为电话访谈的认知状态(TICS)评分β -1.53, 95%可信区间(CI) -1.87 ~ -1.18。在调整后的模型中,与没有损伤的参与者相比,有VI/CI的参与者更有可能在180天死亡(风险比1.61,95% CI 1.10-2.37),并且经历ADL下降(优势比2.11,95% CI 1.39-3.21)。在AMI住院的老年人中,合并症CIs和VIs与高死亡率和出院后残疾恶化有关。未来的研究应该评估在AMI表现期间适应这些损伤的方案,并优化决策和结果。




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
