{"title":"Do liver metastases from gastric cancer contraindicate aggressive surgical resection? A 14-year single-center experience.","authors":"Takefumi Yazawa, Tomohide Hori, Hidekazu Yamamoto, Hideki Harada, Michihiro Yamamoto, Masahiro Yamada, Masaki Tani, Asahi Sato, Yasuyuki Kamada, Ryotaro Tani, Ryuhei Aoyama, Yudai Sasaki, Masazumi Zaima","doi":"10.4292/wjgpt.v11.i5.110","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Advanced gastric cancer (GC) with liver metastasis is often characterized by multiple and bilobular metastases and may also be associated with extrahepatic metastatic lesions. Hence, many physicians consider that radical surgeries are contraindicated for liver metastases from GC (LMGC). According to the 2017 Japanese treatment guideline for GC, a smaller number of liver metastases without unresectable factors may be an indication for liver resection (LR) with curability. The actual 5-year overall survival (OS) rate ranges from 0 to 0.37.</p><p><strong>Aim: </strong>To present the institutional indications for LR for LMGC and identify important factors for prognostic outcomes.</p><p><strong>Methods: </strong>In total, 30 patients underwent LR for LMGC during a 14-year period, and we evaluated the clinical, surgical, and oncological findings. In all patients, radical surgery with intentional lymphadenectomy was performed for the primary GC. The median follow-up duration after the initial LR was 33.7 mo, and three patients with no recurrence died of causes unrelated to the LMGC. The OS and recurrence-free survival rates after the initial LR were assessed.</p><p><strong>Results: </strong>Seventeen patients had metachronous LMGC. The initial LR achieved curability in 29 patients. Perioperative chemotherapy was introduced in 23 patients. The median greatest LMGC dimension was 30 mm, and the median number of LMGC was two. Twenty-two patients had unilobular LMGC. The 5-year OS and recurrence-free survival rates were 0.48 and 0.28, respectively. The median survival duration and recurrence-free duration after the initial LR were 16.8 and 8.6 mo, respectively. Twenty-one patients developed recurrence after the initial LR. Additional surgeries for recurrence were performed in nine patients, and these surgeries clearly prolonged the patients' survival. Pathological serosal invasion was an independent predictor of a poor prognostic outcome after the initial LR. Aggressive LR may be indicated for carefully selected patients with LMGC.</p><p><strong>Conclusion: </strong>Our results of LR for LMGC seem acceptable. Additional surgeries for recurrence after the initial LR might prolong OS. Pathological serosal invasion is important for poor prognostic outcomes.</p>","PeriodicalId":23755,"journal":{"name":"World Journal of Gastrointestinal Pharmacology and Therapeutics","volume":"11 5","pages":"110-122"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a3/75/WJGPT-11-110.PMC7667407.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Pharmacology and Therapeutics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4292/wjgpt.v11.i5.110","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Advanced gastric cancer (GC) with liver metastasis is often characterized by multiple and bilobular metastases and may also be associated with extrahepatic metastatic lesions. Hence, many physicians consider that radical surgeries are contraindicated for liver metastases from GC (LMGC). According to the 2017 Japanese treatment guideline for GC, a smaller number of liver metastases without unresectable factors may be an indication for liver resection (LR) with curability. The actual 5-year overall survival (OS) rate ranges from 0 to 0.37.
Aim: To present the institutional indications for LR for LMGC and identify important factors for prognostic outcomes.
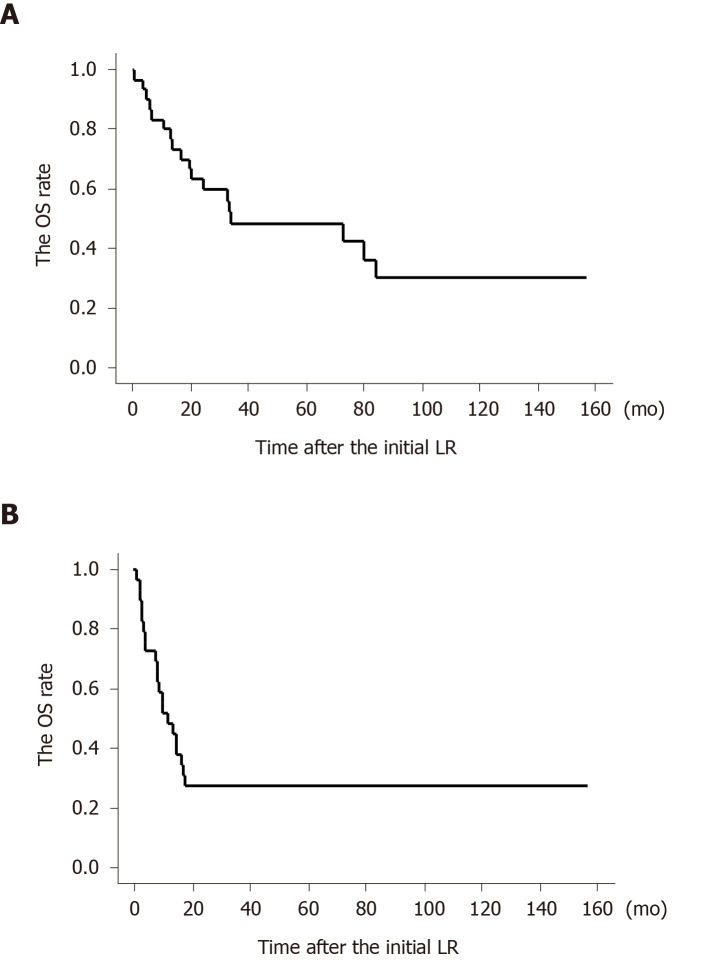
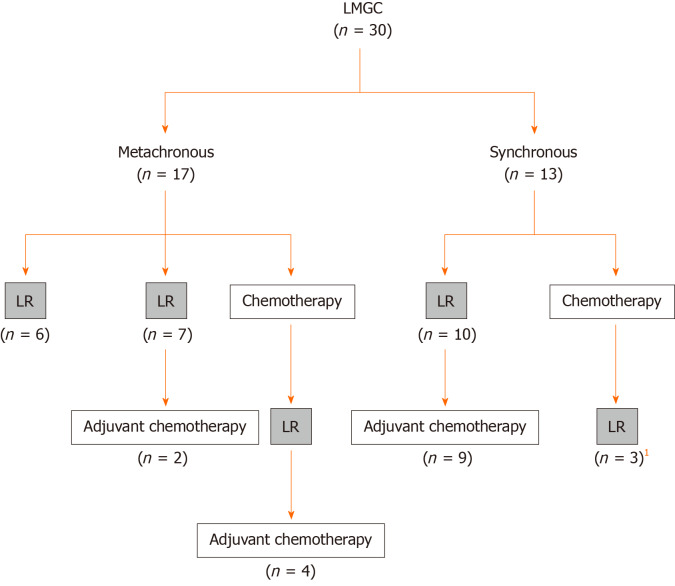
Methods: In total, 30 patients underwent LR for LMGC during a 14-year period, and we evaluated the clinical, surgical, and oncological findings. In all patients, radical surgery with intentional lymphadenectomy was performed for the primary GC. The median follow-up duration after the initial LR was 33.7 mo, and three patients with no recurrence died of causes unrelated to the LMGC. The OS and recurrence-free survival rates after the initial LR were assessed.
Results: Seventeen patients had metachronous LMGC. The initial LR achieved curability in 29 patients. Perioperative chemotherapy was introduced in 23 patients. The median greatest LMGC dimension was 30 mm, and the median number of LMGC was two. Twenty-two patients had unilobular LMGC. The 5-year OS and recurrence-free survival rates were 0.48 and 0.28, respectively. The median survival duration and recurrence-free duration after the initial LR were 16.8 and 8.6 mo, respectively. Twenty-one patients developed recurrence after the initial LR. Additional surgeries for recurrence were performed in nine patients, and these surgeries clearly prolonged the patients' survival. Pathological serosal invasion was an independent predictor of a poor prognostic outcome after the initial LR. Aggressive LR may be indicated for carefully selected patients with LMGC.
Conclusion: Our results of LR for LMGC seem acceptable. Additional surgeries for recurrence after the initial LR might prolong OS. Pathological serosal invasion is important for poor prognostic outcomes.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
