Laura K Stein, Alana Kornspun, John Erdman, Mandip S Dhamoon
{"title":"Readmissions for Depression and Suicide Attempt following Stroke and Myocardial Infarction.","authors":"Laura K Stein, Alana Kornspun, John Erdman, Mandip S Dhamoon","doi":"10.1159/000509454","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>Rates of depression after ischemic stroke (IS) and myocardial infarction (MI) are significantly higher than in the general population and associated with morbidity and mortality. There is a lack of nationally representative data comparing depression and suicide attempt (SA) after these distinct ischemic vascular events.</p><p><strong>Methods: </strong>The 2013 Nationwide Readmissions Database contains >14 million US admissions for all payers and the uninsured. Using International Classification of Disease, 9th Revision, Clinical Modification Codes, we identified index admission with IS (n = 434,495) or MI (n = 539,550) and readmission for depression or SA. We calculated weighted frequencies of readmission. We performed adjusted Cox regression to calculate hazard ratio (HR) for readmission for depression and SA up to 1 year following IS versus MI. Analyses were stratified by discharge home versus elsewhere.</p><p><strong>Results: </strong>Weighted depression readmission rates were higher at 30, 60, and 90 days in patients with IS versus MI (0.04%, 0.09%, 0.12% vs. 0.03%, 0.05%, 0.07%, respectively). There was no significant difference in SA readmissions between groups. The adjusted HR for readmission due to depression was 1.49 for IS versus MI (95% CI 1.25-1.79, p < 0.0001). History of depression (HR 3.70 [3.07-4.46]), alcoholism (2.04 [1.34-3.09]), and smoking (1.38 [1.15-1.64]) were associated with increased risk of depression readmission. Age >70 years (0.46 [0.37-0.56]) and discharge home (0.69 [0.57-0.83]) were associated with reduced hazards of readmission due to depression.</p><p><strong>Conclusions: </strong>IS was associated with greater hazard of readmission due to depression compared to MI. Patients with a history of depression, smoking, and alcoholism were more likely to be readmitted with depression, while advanced age and discharge home were protective. It is unclear to what extent differences in type of ischemic tissue damage and disability contribute, and further investigation is warranted.</p>","PeriodicalId":45709,"journal":{"name":"Cerebrovascular Diseases Extra","volume":"10 2","pages":"94-104"},"PeriodicalIF":2.1000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1159/000509454","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cerebrovascular Diseases Extra","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000509454","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/8/27 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 3
Abstract
Background and purpose: Rates of depression after ischemic stroke (IS) and myocardial infarction (MI) are significantly higher than in the general population and associated with morbidity and mortality. There is a lack of nationally representative data comparing depression and suicide attempt (SA) after these distinct ischemic vascular events.
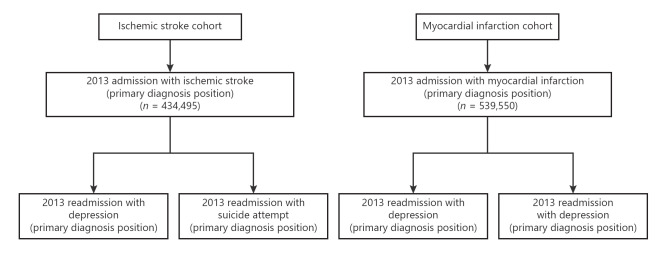
Methods: The 2013 Nationwide Readmissions Database contains >14 million US admissions for all payers and the uninsured. Using International Classification of Disease, 9th Revision, Clinical Modification Codes, we identified index admission with IS (n = 434,495) or MI (n = 539,550) and readmission for depression or SA. We calculated weighted frequencies of readmission. We performed adjusted Cox regression to calculate hazard ratio (HR) for readmission for depression and SA up to 1 year following IS versus MI. Analyses were stratified by discharge home versus elsewhere.
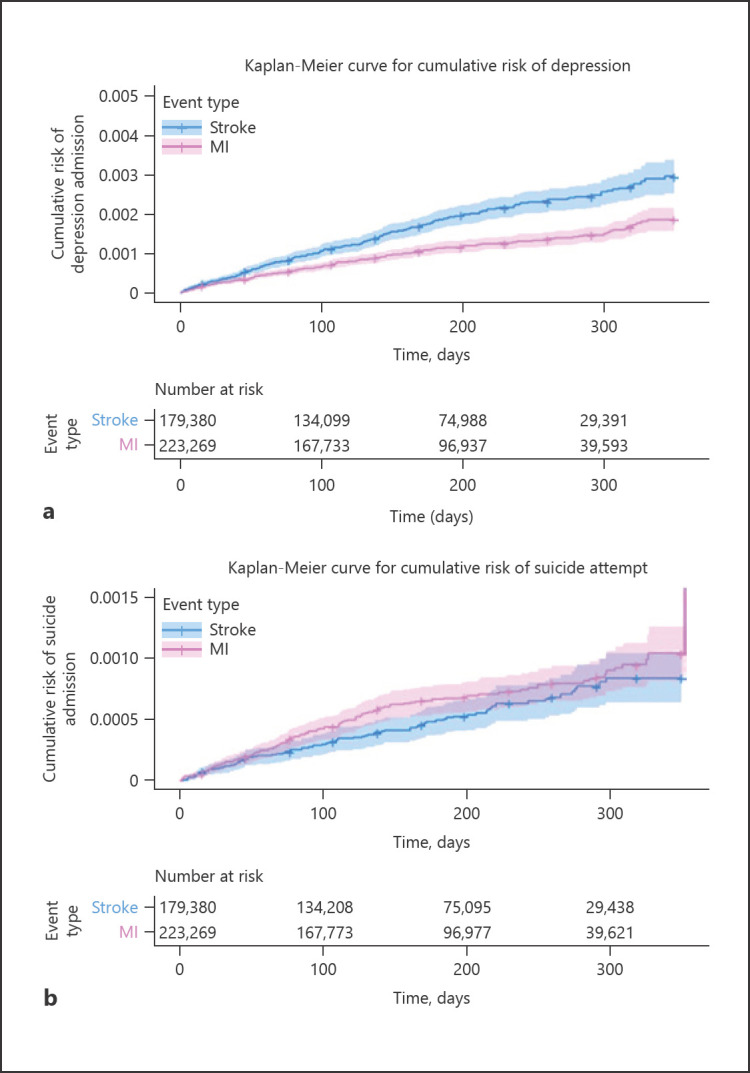
Results: Weighted depression readmission rates were higher at 30, 60, and 90 days in patients with IS versus MI (0.04%, 0.09%, 0.12% vs. 0.03%, 0.05%, 0.07%, respectively). There was no significant difference in SA readmissions between groups. The adjusted HR for readmission due to depression was 1.49 for IS versus MI (95% CI 1.25-1.79, p < 0.0001). History of depression (HR 3.70 [3.07-4.46]), alcoholism (2.04 [1.34-3.09]), and smoking (1.38 [1.15-1.64]) were associated with increased risk of depression readmission. Age >70 years (0.46 [0.37-0.56]) and discharge home (0.69 [0.57-0.83]) were associated with reduced hazards of readmission due to depression.
Conclusions: IS was associated with greater hazard of readmission due to depression compared to MI. Patients with a history of depression, smoking, and alcoholism were more likely to be readmitted with depression, while advanced age and discharge home were protective. It is unclear to what extent differences in type of ischemic tissue damage and disability contribute, and further investigation is warranted.
期刊介绍:
This open access and online-only journal publishes original articles covering the entire spectrum of stroke and cerebrovascular research, drawing from a variety of specialties such as neurology, internal medicine, surgery, radiology, epidemiology, cardiology, hematology, psychology and rehabilitation. Offering an international forum, it meets the growing need for sophisticated, up-to-date scientific information on clinical data, diagnostic testing, and therapeutic issues. The journal publishes original contributions, reviews of selected topics as well as clinical investigative studies. All aspects related to clinical advances are considered, while purely experimental work appears only if directly relevant to clinical issues. Cerebrovascular Diseases Extra provides additional contents based on reviewed and accepted submissions to the main journal Cerebrovascular Diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
