Mona Bischoff-Jung, Elias Flockerzi, Andrea Hasenfus, Arne Viestenz, Pinio Matoula, Ursula Schlötzer-Schrehardt, Berthold Seitz
{"title":"Recurrence of macular corneal dystrophy on the graft 50 years after penetrating keratoplasty.","authors":"Mona Bischoff-Jung, Elias Flockerzi, Andrea Hasenfus, Arne Viestenz, Pinio Matoula, Ursula Schlötzer-Schrehardt, Berthold Seitz","doi":"10.3205/oc000161","DOIUrl":null,"url":null,"abstract":"<p><p><b>Purpose:</b> To report the recurrence of a macular corneal stromal dystrophy 50 years after penetrating keratoplasty (PKP). <b>Methods:</b> Observational case report <b>Case</b> <b>description:</b> A 76-year-old male patient presented with visual impairment in the right eye (OD) 50 years after PKP in 1962 (44 years after PKP also in the left eye (OS) in 1968) following explosion injury. His visual acuity had already been impaired before the trauma because of bilateral corneal opacities. The central corneal thickness of the graft measured 584 µm (OD) and 544 µm (OS), whilst the peripheral host thickness (8 mm zone), however, was 1233 µm (OD, cranial) and 1131 µm (OS, nasal). The original graft diameter measured 6 mm in both eyes and the recipient cornea was cloudy and gray. The endothelial cell count was measured centrally (OD 1162 c/mm<sup>2</sup>, OS 1320 c/mm<sup>2</sup>). The visual acuity was 20/100 (OD) and 20/40 (OS). After excimerlaser-assisted repeated PKP (8.0/8.1 mm, OD), the histological analysis of the former graft revealed deposits of acid mucopolysaccharides (AMP) subepithelially, within the interface, in the donor stroma, and in the endothelium, which proved the peripheral recurrence of a macular corneal stromal dystrophy on the graft. <b>Conclusion:</b> Recurrence of macular corneal stromal dystrophy is seldom, but it may occur many decades after PKP. In this patient, the host's stroma was twice as thick as that of the graft. This may be caused by the active production of acid mucopolysaccharides in the host endothelium with secondary endothelial decompensation. Thus, PKP remains the gold standard in the cure of macular corneal dystrophy for long-term visual rehabilitation.</p>","PeriodicalId":73178,"journal":{"name":"GMS ophthalmology cases","volume":"10 ","pages":"Doc34"},"PeriodicalIF":0.0000,"publicationDate":"2020-08-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7452946/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"GMS ophthalmology cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3205/oc000161","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
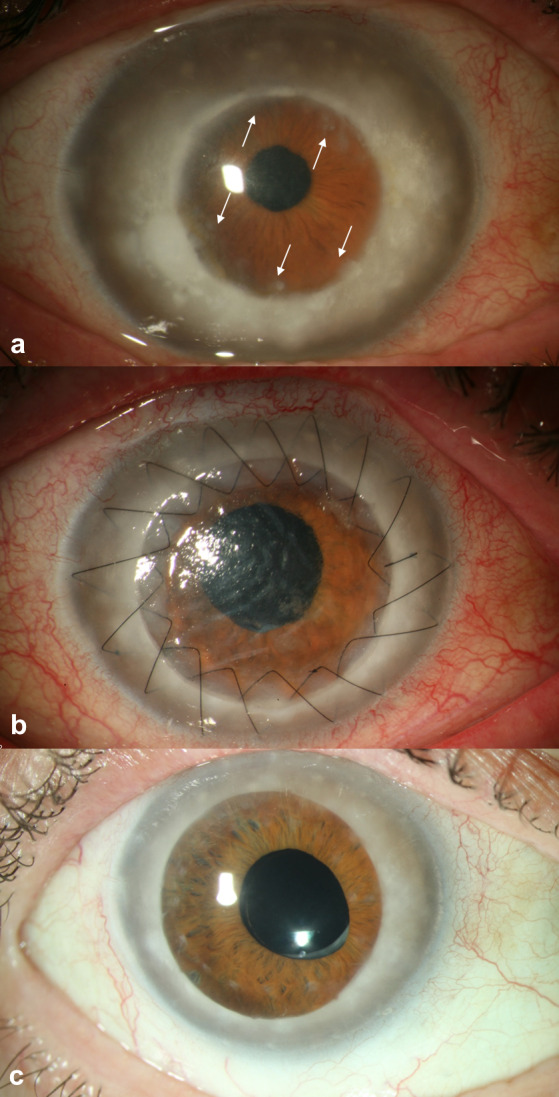
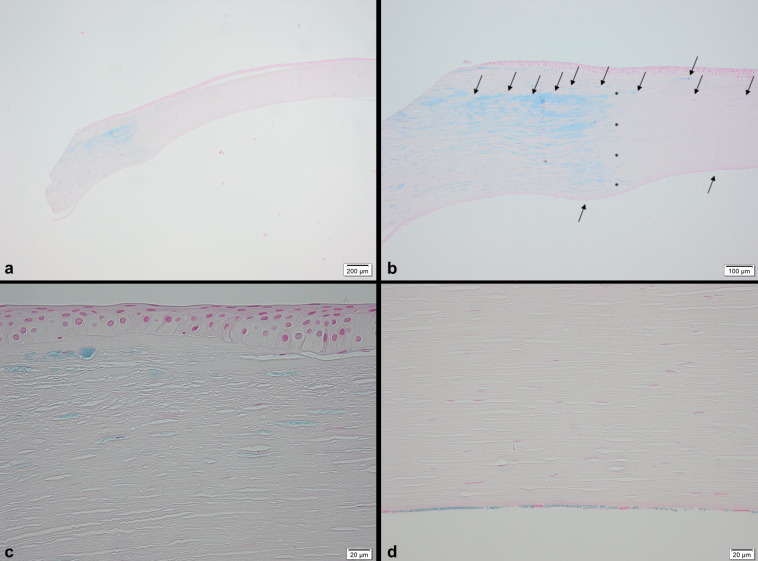
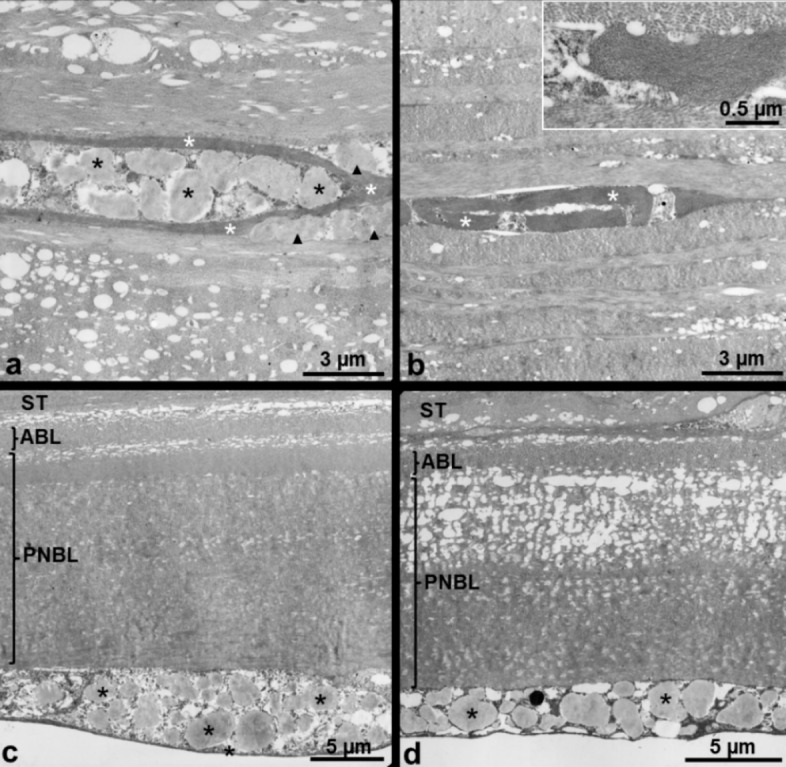
Purpose: To report the recurrence of a macular corneal stromal dystrophy 50 years after penetrating keratoplasty (PKP). Methods: Observational case report Casedescription: A 76-year-old male patient presented with visual impairment in the right eye (OD) 50 years after PKP in 1962 (44 years after PKP also in the left eye (OS) in 1968) following explosion injury. His visual acuity had already been impaired before the trauma because of bilateral corneal opacities. The central corneal thickness of the graft measured 584 µm (OD) and 544 µm (OS), whilst the peripheral host thickness (8 mm zone), however, was 1233 µm (OD, cranial) and 1131 µm (OS, nasal). The original graft diameter measured 6 mm in both eyes and the recipient cornea was cloudy and gray. The endothelial cell count was measured centrally (OD 1162 c/mm2, OS 1320 c/mm2). The visual acuity was 20/100 (OD) and 20/40 (OS). After excimerlaser-assisted repeated PKP (8.0/8.1 mm, OD), the histological analysis of the former graft revealed deposits of acid mucopolysaccharides (AMP) subepithelially, within the interface, in the donor stroma, and in the endothelium, which proved the peripheral recurrence of a macular corneal stromal dystrophy on the graft. Conclusion: Recurrence of macular corneal stromal dystrophy is seldom, but it may occur many decades after PKP. In this patient, the host's stroma was twice as thick as that of the graft. This may be caused by the active production of acid mucopolysaccharides in the host endothelium with secondary endothelial decompensation. Thus, PKP remains the gold standard in the cure of macular corneal dystrophy for long-term visual rehabilitation.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
