{"title":"Peritoneal dialysis in an adult patient with tetralogy of Fallot diagnosed with incomplete Alagille syndrome.","authors":"Malgorzata Ponikowska, Agnieszka Pollak, Ewa Kotwica-Strzalek, Dorota Brodowska-Kania, Magdalena Mosakowska, Rafal Ploski, Stanislaw Niemczyk","doi":"10.1186/s12881-020-01134-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Alagille syndrome is an autosomal dominant disorder usually caused by pathogenic variants of the JAG1 gene. In the past, cholestasis was a condition sine qua non for diagnosis of the syndrome. However, recent advancements in genetic testing have revealed that clinical presentations vary from lack of symptoms, to multiorgan involvement. Tetralogy of Fallot, the most frequent complex congenital heart defect in Alagille Syndrome, very rarely leads to renal failure requiring dialysis - there are only single reports of such cases in the literature, with none of them in Alagille Syndrome.</p><p><strong>Case presentation: </strong>A 41-year-old woman suffering from cyanosis, dyspnea and plethora was admitted to the hospital. The patient suffered from chronic kidney disease and tetralogy of Fallot and had been treated palliatively with Blalock-Taussig shunts in the past; at admission, only minimal flow through the left shunt was preserved. These symptoms, together with impaired mental status and dysmorphic facial features, led to extensive clinical and genetic testing including whole exome sequencing. A previously unknown missense variant c.587G > A within the JAG1 gene was identified. As there were no signs of cholestasis, and subclinical liver involvement was only suggested by elevated alkaline phosphatase levels, the patient was diagnosed with incomplete Alagille Syndrome. End-stage renal disease required introduction of renal replacement therapy. Continuous ambulatory peritoneal dialysis was chosen and the patient's quality of life significantly increased. However, after refusal of further treatment, the patient died at the age of 45.</p><p><strong>Conclusions: </strong>Tetralogy of Fallot should always urge clinicians to evaluate for Alagille Syndrome and offer patients early nephrological care. Although tetralogy of Fallot rarely leads to end-stage renal disease requiring dialysis, if treated palliatively and combined with renal dysplasia (typical of Alagille Syndrome), it can result in severe renal failure as in the presented case. There is no standard treatment for such cases, but based on our experience, peritoneal dialysis is worth consideration. Finally, clinical criteria for the diagnosis of Alagille Syndrome require revision. Previously, diagnosis was based on cholestasis - however, cardiovascular anomalies are found to be more prevalent. Furthermore, the criteria do not include renal impairment, which is also common.</p>","PeriodicalId":9015,"journal":{"name":"BMC Medical Genetics","volume":" ","pages":"195"},"PeriodicalIF":0.0000,"publicationDate":"2020-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s12881-020-01134-7","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Medical Genetics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12881-020-01134-7","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Alagille syndrome is an autosomal dominant disorder usually caused by pathogenic variants of the JAG1 gene. In the past, cholestasis was a condition sine qua non for diagnosis of the syndrome. However, recent advancements in genetic testing have revealed that clinical presentations vary from lack of symptoms, to multiorgan involvement. Tetralogy of Fallot, the most frequent complex congenital heart defect in Alagille Syndrome, very rarely leads to renal failure requiring dialysis - there are only single reports of such cases in the literature, with none of them in Alagille Syndrome.
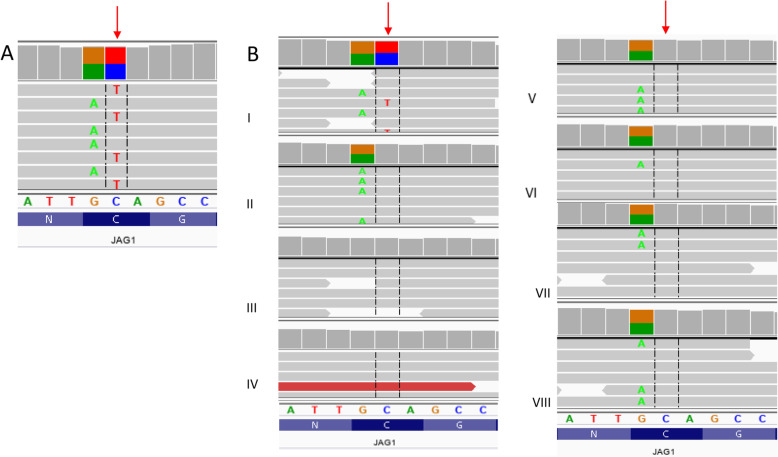
Case presentation: A 41-year-old woman suffering from cyanosis, dyspnea and plethora was admitted to the hospital. The patient suffered from chronic kidney disease and tetralogy of Fallot and had been treated palliatively with Blalock-Taussig shunts in the past; at admission, only minimal flow through the left shunt was preserved. These symptoms, together with impaired mental status and dysmorphic facial features, led to extensive clinical and genetic testing including whole exome sequencing. A previously unknown missense variant c.587G > A within the JAG1 gene was identified. As there were no signs of cholestasis, and subclinical liver involvement was only suggested by elevated alkaline phosphatase levels, the patient was diagnosed with incomplete Alagille Syndrome. End-stage renal disease required introduction of renal replacement therapy. Continuous ambulatory peritoneal dialysis was chosen and the patient's quality of life significantly increased. However, after refusal of further treatment, the patient died at the age of 45.
Conclusions: Tetralogy of Fallot should always urge clinicians to evaluate for Alagille Syndrome and offer patients early nephrological care. Although tetralogy of Fallot rarely leads to end-stage renal disease requiring dialysis, if treated palliatively and combined with renal dysplasia (typical of Alagille Syndrome), it can result in severe renal failure as in the presented case. There is no standard treatment for such cases, but based on our experience, peritoneal dialysis is worth consideration. Finally, clinical criteria for the diagnosis of Alagille Syndrome require revision. Previously, diagnosis was based on cholestasis - however, cardiovascular anomalies are found to be more prevalent. Furthermore, the criteria do not include renal impairment, which is also common.
期刊介绍:
BMC Medical Genetics is an open access journal publishing original peer-reviewed research articles in the effects of genetic variation in individuals, families and among populations in relation to human health and disease.
Note: BMC Medical Genetics is now closed. This journal has merged with BMC Medical Genomics, a broad-scope, open access community journal for all medical genetics and genomics research.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
