Findings on intraprocedural non-contrast computed tomographic imaging following hepatic artery embolization are associated with development of contrast-induced nephropathy.
Mohamed M Soliman, Debkumar Sarkar, Ilya Glezerman, Majid Maybody
{"title":"Findings on intraprocedural non-contrast computed tomographic imaging following hepatic artery embolization are associated with development of contrast-induced nephropathy.","authors":"Mohamed M Soliman, Debkumar Sarkar, Ilya Glezerman, Majid Maybody","doi":"10.5527/wjn.v9.i2.33","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Contrast-induced nephropathy (CIN) is a reversible form of acute kidney injury that occurs within 48-72 h of exposure to intravascular contrast material. CIN is the third leading cause of hospital-acquired acute kidney injury and accounts for 12% of such cases. Risk factors for CIN development can be divided into patient- and procedure-related. The former includes pre-existing chronic renal insufficiency and diabetes mellitus. The latter includes high contrast volume and repeated exposure over 72 h. The incidence of CIN is relatively low (up to 5%) in patients with intact renal function. However, in patients with known chronic renal insufficiency, the incidence can reach up to 27%.</p><p><strong>Aim: </strong>To examine the association between renal enhancement pattern on non-contrast enhanced computed tomographic (CT) images obtained immediately following hepatic artery embolization with development of CIN.</p><p><strong>Methods: </strong>Retrospective review of all patients who underwent hepatic artery embolization between 01/2010 and 01/2011 (<i>n</i> = 162) was performed. Patients without intraprocedural CT imaging (<i>n</i> = 51), combined embolization/ablation (<i>n</i> = 6) and those with chronic kidney disease (<i>n</i> = 21) were excluded. The study group comprised of 84 patients with 106 procedures. CIN was defined as 25% increase above baseline serum creatinine or absolute increase ≥ 0.5 mg/dL within 72 h post-embolization. Post-embolization CT was reviewed for renal enhancement patterns and presence of renal artery calcifications. The association between non-contrast CT findings and CIN development was examined by Fisher's Exact Test.</p><p><strong>Results: </strong>CIN occurred in 11/106 (10.3%) procedures (Group A, <i>n</i> = 10). The renal enhancement pattern in patients who did not experience CIN (Group B, <i>n</i> = 74 with 95/106 procedures) was late excretory in 93/95 (98%) and early excretory (EE) in 2/95 (2%). However, in Group A, there was a significantly higher rate of EE pattern (6/11, 55%) compared to late excretory pattern (5/11) (<i>P</i> < 0.001). A significantly higher percentage of patients that developed CIN had renal artery calcifications (6/11 <i>vs</i> 20/95, 55% <i>vs</i> 21%, <i>P</i> = 0.02).</p><p><strong>Conclusion: </strong>A hyperdense renal parenchyma relative to surrounding skeletal muscle (EE pattern) and presence of renal artery calcifications on immediate post-HAE non-contrast CT images in patients with low risk for CIN are independently associated with CIN development.</p>","PeriodicalId":23745,"journal":{"name":"World Journal of Nephrology","volume":"9 2","pages":"33-42"},"PeriodicalIF":0.0000,"publicationDate":"2020-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/a0/22/WJN-9-33.PMC7701934.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5527/wjn.v9.i2.33","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Contrast-induced nephropathy (CIN) is a reversible form of acute kidney injury that occurs within 48-72 h of exposure to intravascular contrast material. CIN is the third leading cause of hospital-acquired acute kidney injury and accounts for 12% of such cases. Risk factors for CIN development can be divided into patient- and procedure-related. The former includes pre-existing chronic renal insufficiency and diabetes mellitus. The latter includes high contrast volume and repeated exposure over 72 h. The incidence of CIN is relatively low (up to 5%) in patients with intact renal function. However, in patients with known chronic renal insufficiency, the incidence can reach up to 27%.
Aim: To examine the association between renal enhancement pattern on non-contrast enhanced computed tomographic (CT) images obtained immediately following hepatic artery embolization with development of CIN.
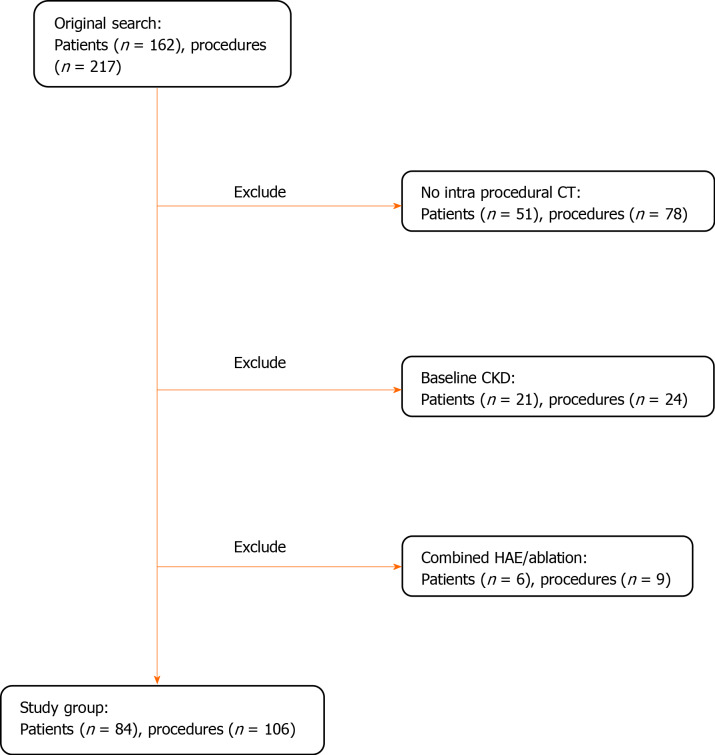
Methods: Retrospective review of all patients who underwent hepatic artery embolization between 01/2010 and 01/2011 (n = 162) was performed. Patients without intraprocedural CT imaging (n = 51), combined embolization/ablation (n = 6) and those with chronic kidney disease (n = 21) were excluded. The study group comprised of 84 patients with 106 procedures. CIN was defined as 25% increase above baseline serum creatinine or absolute increase ≥ 0.5 mg/dL within 72 h post-embolization. Post-embolization CT was reviewed for renal enhancement patterns and presence of renal artery calcifications. The association between non-contrast CT findings and CIN development was examined by Fisher's Exact Test.
Results: CIN occurred in 11/106 (10.3%) procedures (Group A, n = 10). The renal enhancement pattern in patients who did not experience CIN (Group B, n = 74 with 95/106 procedures) was late excretory in 93/95 (98%) and early excretory (EE) in 2/95 (2%). However, in Group A, there was a significantly higher rate of EE pattern (6/11, 55%) compared to late excretory pattern (5/11) (P < 0.001). A significantly higher percentage of patients that developed CIN had renal artery calcifications (6/11 vs 20/95, 55% vs 21%, P = 0.02).
Conclusion: A hyperdense renal parenchyma relative to surrounding skeletal muscle (EE pattern) and presence of renal artery calcifications on immediate post-HAE non-contrast CT images in patients with low risk for CIN are independently associated with CIN development.




 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
