Jeong Yun Jang, Jesang Yu, Kye Jin Song, Yoon Young Jo, Ye Jin Yoo, Sung-Bae Kim, Sook Ryun Park, Young-Hee Kim, Hyeong Ryul Kim, Jong Hoon Kim
{"title":"Prognostic significance of lymph node ratio after neoadjuvant chemoradiation therapy for esophageal squamous cell carcinoma.","authors":"Jeong Yun Jang, Jesang Yu, Kye Jin Song, Yoon Young Jo, Ye Jin Yoo, Sung-Bae Kim, Sook Ryun Park, Young-Hee Kim, Hyeong Ryul Kim, Jong Hoon Kim","doi":"10.3857/roj.2020.00850","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We retrospectively evaluated the prognostic significance of lymph node ratio (LNR) in patients with esophageal squamous cell carcinoma who underwent neoadjuvant concurrent chemoradiation therapy (NCRT) followed by surgery.</p><p><strong>Materials and methods: </strong>In total, 270 patients who underwent NCRT followed by surgery between August 2005 and December 2015 were included. They were divided into three groups: LNR 0 (n = 196), LNR low (0 < LNR ≤ 0.1; n = 63), and LNR high (>0.1; n = 11). The primary endpoint was overall survival (OS), and the secondary endpoints were freedom from local recurrence (FFLR), distant metastasis-free survival (DMFS), and disease-free survival (DFS).</p><p><strong>Results: </strong>The median number of retrieved lymph nodes per patient was 33. Pathologically, 74 patients had positive lymph nodes. The median follow-up duration was 36.1 months, and the median survival period was 68.4 months. There was a significant correlation between LNR and the number of positive lymph nodes (correlation coefficient = 0.763, p < 0.001). There was a substantial difference in the OS among the LNR groups, with 2-year survival rates of 79.0%, 54.0%, and 9.1% in the LNR 0, LNR low, and LNR high groups, respectively (p < 0.001). A marked decrease in FFLP, DMFS, and DFS was observed with the increasing LNR. In subgroup analysis, the survival results of patients with clinically positive lymph node were similar from those of entire cohort.</p><p><strong>Conclusion: </strong>LNR is a significant prognostic factor in patients with esophageal squamous cell carcinoma who underwent NCRT followed by surgery. Additional treatment and closer follow-up would be necessary for patients with a high LNR.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"38 4","pages":"244-252"},"PeriodicalIF":2.2000,"publicationDate":"2020-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/67/33/roj-2020-00850.PMC7785840.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2020.00850","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/11/25 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: We retrospectively evaluated the prognostic significance of lymph node ratio (LNR) in patients with esophageal squamous cell carcinoma who underwent neoadjuvant concurrent chemoradiation therapy (NCRT) followed by surgery.
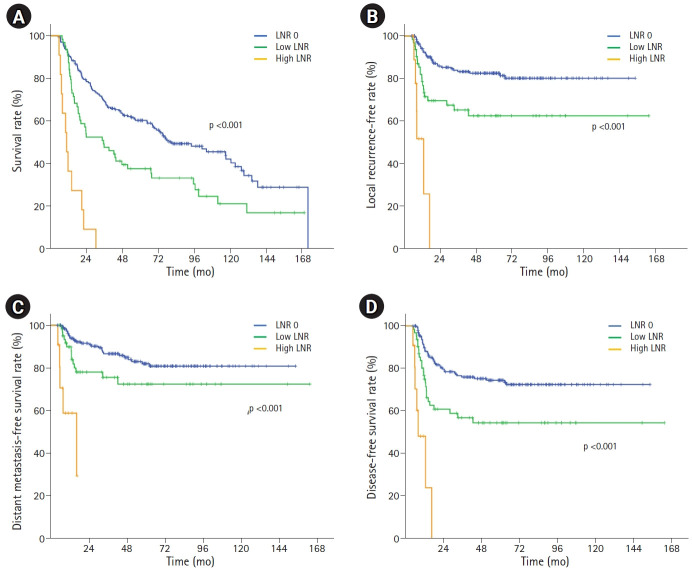
Materials and methods: In total, 270 patients who underwent NCRT followed by surgery between August 2005 and December 2015 were included. They were divided into three groups: LNR 0 (n = 196), LNR low (0 < LNR ≤ 0.1; n = 63), and LNR high (>0.1; n = 11). The primary endpoint was overall survival (OS), and the secondary endpoints were freedom from local recurrence (FFLR), distant metastasis-free survival (DMFS), and disease-free survival (DFS).
Results: The median number of retrieved lymph nodes per patient was 33. Pathologically, 74 patients had positive lymph nodes. The median follow-up duration was 36.1 months, and the median survival period was 68.4 months. There was a significant correlation between LNR and the number of positive lymph nodes (correlation coefficient = 0.763, p < 0.001). There was a substantial difference in the OS among the LNR groups, with 2-year survival rates of 79.0%, 54.0%, and 9.1% in the LNR 0, LNR low, and LNR high groups, respectively (p < 0.001). A marked decrease in FFLP, DMFS, and DFS was observed with the increasing LNR. In subgroup analysis, the survival results of patients with clinically positive lymph node were similar from those of entire cohort.
Conclusion: LNR is a significant prognostic factor in patients with esophageal squamous cell carcinoma who underwent NCRT followed by surgery. Additional treatment and closer follow-up would be necessary for patients with a high LNR.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
