{"title":"Role of the Bronchoalveolar Lavage in Noncritically Ill Patients during the SARS-CoV-2 Epidemic.","authors":"Olivier Taton, Emmanuelle Papleux, Benjamin Bondue, Christiane Knoop, Sébastien Van Laethem, Alain Bauler, Delphine Martiny, Isabel Montesinos, Marie-Luce Delforge, Kahina Elmaouhab, Dimitri Leduc","doi":"10.1155/2020/9012187","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bronchoalveolar lavage (BAL) is currently not recommended in noncritically ill patients for the diagnosis of SARS-CoV-2 infection. Indeed, the diagnosis is based on the RT-PCR test on a nasopharyngeal swab (NPS) and abnormal findings on the chest CT scan. However, the sensitivity of the NPS and the specificity of the chest CT scan are low. Results of BAL in case of negative NPS testing are underreported, especially in the subgroup of immunocompromised patients.</p><p><strong>Objectives: </strong>The added value of BAL in the management of unstable, but noncritically ill patients, suspected of having SARS-CoV-2 infection despite one previous negative NPS and the side effects of the procedure for the patients and the health-care providers, were assessed during the epidemic peak of the COVID-19 outbreak in Belgium.</p><p><strong>Methods: </strong>This multicentric study included all consecutive noncritically ill patients hospitalized with a clinical and radiological suspicion of SARS-CoV-2 infection but with a negative NPS. BAL was performed according to a predefined decisional algorithm based on their state of immunocompetence, the chest CT scan features, and their respiratory status.</p><p><strong>Results: </strong>Among the 55 patients included in the study, 14 patients were diagnosed with a SARS-CoV-2 infection. Interestingly, there was a relationship between the cycle threshold of the RT-PCR and the interval of time between the symptom onset and the BAL procedure (Pearson's correlation coefficient = 0.8, <i>p</i> = 0.0004). Therapeutic management was changed in 33 patients because another infectious agent was identified in 23 patients or because an alternative diagnosis was made in 10 patients. In immunocompromised patients, the impact of BAL was even more marked (change in therapy for 13/17 patients). No significant adverse event was noted for patients or health-care staff. All health-care workers remained negative for SARS-CoV-2 NPS and serology at the end of the study.</p><p><strong>Conclusions: </strong>In this real-life study, BAL can be performed safely in selected noncritically ill patients suspected of SARS-CoV-2 infection, providing significant clinical benefits that outweigh the risks.</p>","PeriodicalId":46434,"journal":{"name":"Pulmonary Medicine","volume":"2020 ","pages":"9012187"},"PeriodicalIF":2.1000,"publicationDate":"2020-12-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/9012187","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/9012187","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 6
Abstract
Background: Bronchoalveolar lavage (BAL) is currently not recommended in noncritically ill patients for the diagnosis of SARS-CoV-2 infection. Indeed, the diagnosis is based on the RT-PCR test on a nasopharyngeal swab (NPS) and abnormal findings on the chest CT scan. However, the sensitivity of the NPS and the specificity of the chest CT scan are low. Results of BAL in case of negative NPS testing are underreported, especially in the subgroup of immunocompromised patients.
Objectives: The added value of BAL in the management of unstable, but noncritically ill patients, suspected of having SARS-CoV-2 infection despite one previous negative NPS and the side effects of the procedure for the patients and the health-care providers, were assessed during the epidemic peak of the COVID-19 outbreak in Belgium.
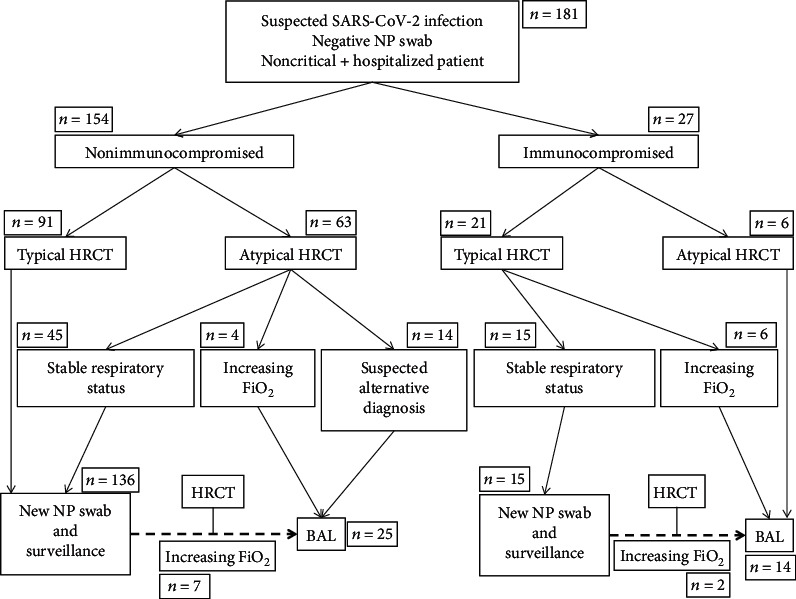
Methods: This multicentric study included all consecutive noncritically ill patients hospitalized with a clinical and radiological suspicion of SARS-CoV-2 infection but with a negative NPS. BAL was performed according to a predefined decisional algorithm based on their state of immunocompetence, the chest CT scan features, and their respiratory status.
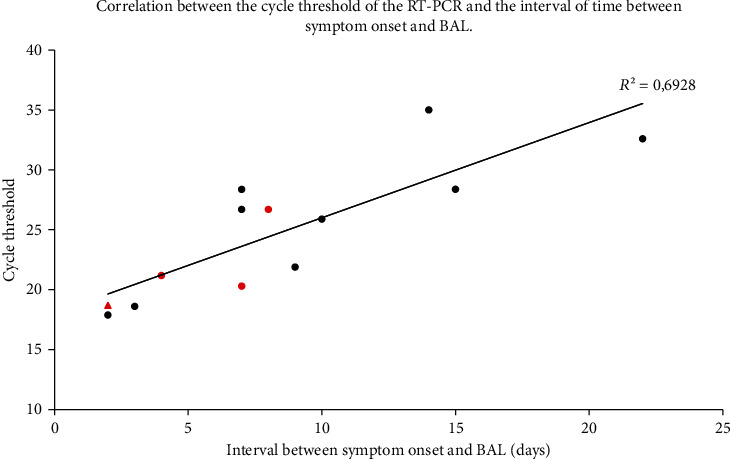
Results: Among the 55 patients included in the study, 14 patients were diagnosed with a SARS-CoV-2 infection. Interestingly, there was a relationship between the cycle threshold of the RT-PCR and the interval of time between the symptom onset and the BAL procedure (Pearson's correlation coefficient = 0.8, p = 0.0004). Therapeutic management was changed in 33 patients because another infectious agent was identified in 23 patients or because an alternative diagnosis was made in 10 patients. In immunocompromised patients, the impact of BAL was even more marked (change in therapy for 13/17 patients). No significant adverse event was noted for patients or health-care staff. All health-care workers remained negative for SARS-CoV-2 NPS and serology at the end of the study.
Conclusions: In this real-life study, BAL can be performed safely in selected noncritically ill patients suspected of SARS-CoV-2 infection, providing significant clinical benefits that outweigh the risks.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
