Young Gon Na, Beom Koo Lee, Ji Uk Choi, Byung Hoon Lee, Jae Ang Sim
{"title":"Change of joint-line convergence angle should be considered for accurate alignment correction in high tibial osteotomy.","authors":"Young Gon Na, Beom Koo Lee, Ji Uk Choi, Byung Hoon Lee, Jae Ang Sim","doi":"10.1186/s43019-020-00076-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The alignment correction after high tibial osteotomy (HTO) is made both by bony correction and soft-tissue correction around the knee. Change of the joint-line convergence angle (JLCA) represents the soft-tissue correction after HTO, which is the angle made by a tangential line between the femoral condyles and the tibial plateau. We described the patterns of JLCA change and related factors after HTO and investigated the appropriate preoperative planning method.</p><p><strong>Methods: </strong>Eighty patients who underwent HTO between 2013 and 2016 were included for this retrospective study. Standing, whole-limb radiograph, supine knee anteroposterior (AP) and lateral were measured on the preoperative and postoperative radiographs. The patterns of JLCA changes and related factors were analyzed.</p><p><strong>Results: </strong>JLCA decreased by a mean of 0.9° ± 1.2° (P < 0.001) after HTO. Sixteen patients (20%, group II) showed a greater JLCA decrease ≥ 2°, while 64 (80%, group I) patients remained in a narrow range of JLCA change < 2°. Group II showed more varus deformity (varus 8.1° vs. varus 4.7° in the mechanical femorotibial angle, P < 0.001), greater JLCA on standing (4.9° vs. 2.1°, P < 0.001), and the difference of JLCA in the standing and supine positions (2.8° vs. 0.7°, P < 0.001) preoperatively compared to group I. The risk of a greater JLCA decrease ≥ 2° was associated with greater preoperative JLCA in the standing position and the difference between the JLCA in the standing and supine positions. Postoperative JLCA correlated better with preoperative JLCA in the supine position than those in the standing position. A preoperative JLCA ≥ 4° or the difference of preoperative JLCA in the standing and supine positions ≥ 1.7° was the cut-off value to predict a large JLCA decrease ≥ 2° after HTO in the receiver operating characteristic (ROC) curve analysis.</p><p><strong>Conclusions: </strong>Surgeons should consider the effect of the JLCA change during the preoperative planning and intraoperative procedure to avoid unintended overcorrection.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":"33 1","pages":"4"},"PeriodicalIF":4.9000,"publicationDate":"2021-01-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s43019-020-00076-x","citationCount":"32","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-020-00076-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 32
Abstract
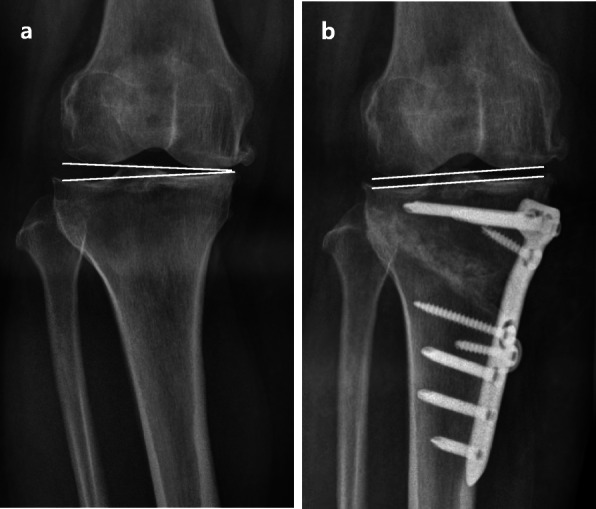
Background: The alignment correction after high tibial osteotomy (HTO) is made both by bony correction and soft-tissue correction around the knee. Change of the joint-line convergence angle (JLCA) represents the soft-tissue correction after HTO, which is the angle made by a tangential line between the femoral condyles and the tibial plateau. We described the patterns of JLCA change and related factors after HTO and investigated the appropriate preoperative planning method.
Methods: Eighty patients who underwent HTO between 2013 and 2016 were included for this retrospective study. Standing, whole-limb radiograph, supine knee anteroposterior (AP) and lateral were measured on the preoperative and postoperative radiographs. The patterns of JLCA changes and related factors were analyzed.
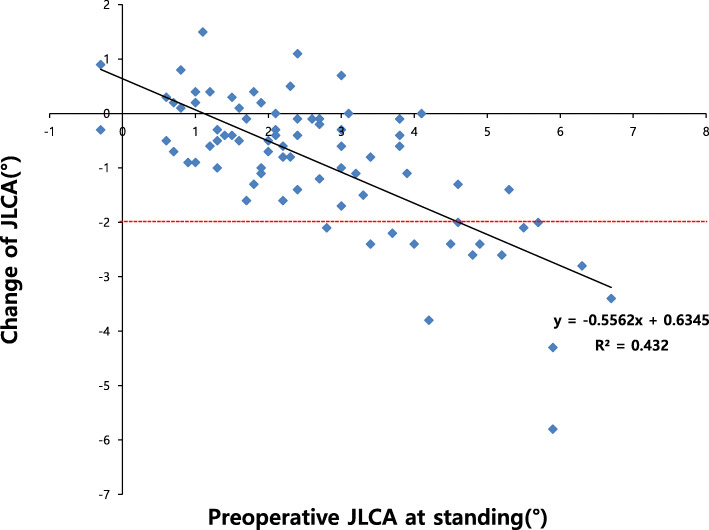
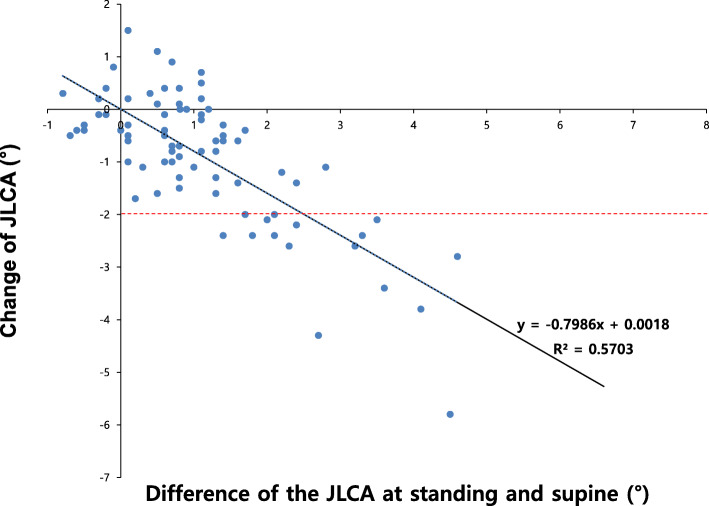
Results: JLCA decreased by a mean of 0.9° ± 1.2° (P < 0.001) after HTO. Sixteen patients (20%, group II) showed a greater JLCA decrease ≥ 2°, while 64 (80%, group I) patients remained in a narrow range of JLCA change < 2°. Group II showed more varus deformity (varus 8.1° vs. varus 4.7° in the mechanical femorotibial angle, P < 0.001), greater JLCA on standing (4.9° vs. 2.1°, P < 0.001), and the difference of JLCA in the standing and supine positions (2.8° vs. 0.7°, P < 0.001) preoperatively compared to group I. The risk of a greater JLCA decrease ≥ 2° was associated with greater preoperative JLCA in the standing position and the difference between the JLCA in the standing and supine positions. Postoperative JLCA correlated better with preoperative JLCA in the supine position than those in the standing position. A preoperative JLCA ≥ 4° or the difference of preoperative JLCA in the standing and supine positions ≥ 1.7° was the cut-off value to predict a large JLCA decrease ≥ 2° after HTO in the receiver operating characteristic (ROC) curve analysis.
Conclusions: Surgeons should consider the effect of the JLCA change during the preoperative planning and intraoperative procedure to avoid unintended overcorrection.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
