Yasmina Serinel , Camilla Hoyos , Ahmad Qasem , Brendon J. Yee , Ronald R. Grunstein , Keith H. Wong , Craig L. Phillips
{"title":"Diurnal changes in central blood pressure and pulse pressure amplification in patients with obstructive sleep apnoea","authors":"Yasmina Serinel , Camilla Hoyos , Ahmad Qasem , Brendon J. Yee , Ronald R. Grunstein , Keith H. Wong , Craig L. Phillips","doi":"10.1016/j.ijchy.2019.100002","DOIUrl":null,"url":null,"abstract":"<div><h3>Study objectives</h3><p>Recent evidence suggests that compared to peripheral blood pressure (BP), central BP may be more strongly associated with target organ damage and cardiovascular morbidity and mortality. Technological advances now allow the ambulatory measurement of peripheral and central BP over 24 h. For the first time, we set out to characterise the diurnal profile of central BP and pulse pressure amplification (PPA) in patients with obstructive sleep apnoea (OSA).</p></div><div><h3>Methods</h3><p>In this observational study, patients with moderate to severe OSA underwent 24 h central and peripheral BP testing before and after at least 4 weeks of CPAP therapy. Concurrent actigraphy was performed to confirm sleep and wake times.</p></div><div><h3>Results</h3><p>36 patients were screened, 31 had successful testing (mean (SD) age 45 ± 10 years, AHI 58 ± 27 events/hr, Office BP 136/89 ± 10.7/9.5 mmHg, 32% on anti-hypertensives, 77% dippers), 21 completed testing post CPAP. Central systolic and diastolic BP followed the same nocturnal dipping profile as peripheral BP, however the peripheral pulse pressure (PP) narrowed in sleep (−3.2 mmHg, p < 0.001), whereas the central PP remained unchanged (0.124 mmHg, NS), causing a significant reduction in PPA overnight (−10.7%, p < 0.001). The magnitude of dip in central systolic pressure was less than peripheral systolic pressure (by 2.3 mmHg, p < 0.001). After treatment with CPAP, the PPA reduction overnight was attenuated (by −3.3%, p = 0.004).</p></div><div><h3>Conclusions</h3><p>In moderate to severe OSA, central BP and PPA reduce overnight during sleep. Further randomised controlled studies are needed to quantify the differential effects of CPAP and anti-hypertensives on central versus peripheral BP.</p></div>","PeriodicalId":36839,"journal":{"name":"International Journal of Cardiology: Hypertension","volume":"1 ","pages":"Article 100002"},"PeriodicalIF":0.0000,"publicationDate":"2019-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijchy.2019.100002","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiology: Hypertension","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590086219300023","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/5/15 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 2
Abstract
Study objectives
Recent evidence suggests that compared to peripheral blood pressure (BP), central BP may be more strongly associated with target organ damage and cardiovascular morbidity and mortality. Technological advances now allow the ambulatory measurement of peripheral and central BP over 24 h. For the first time, we set out to characterise the diurnal profile of central BP and pulse pressure amplification (PPA) in patients with obstructive sleep apnoea (OSA).
Methods
In this observational study, patients with moderate to severe OSA underwent 24 h central and peripheral BP testing before and after at least 4 weeks of CPAP therapy. Concurrent actigraphy was performed to confirm sleep and wake times.
Results
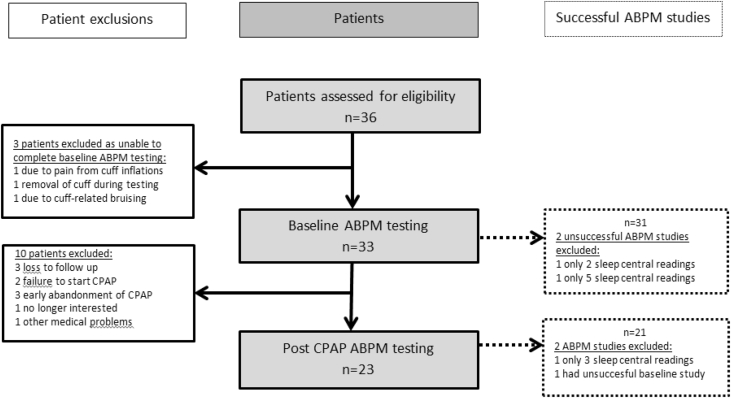
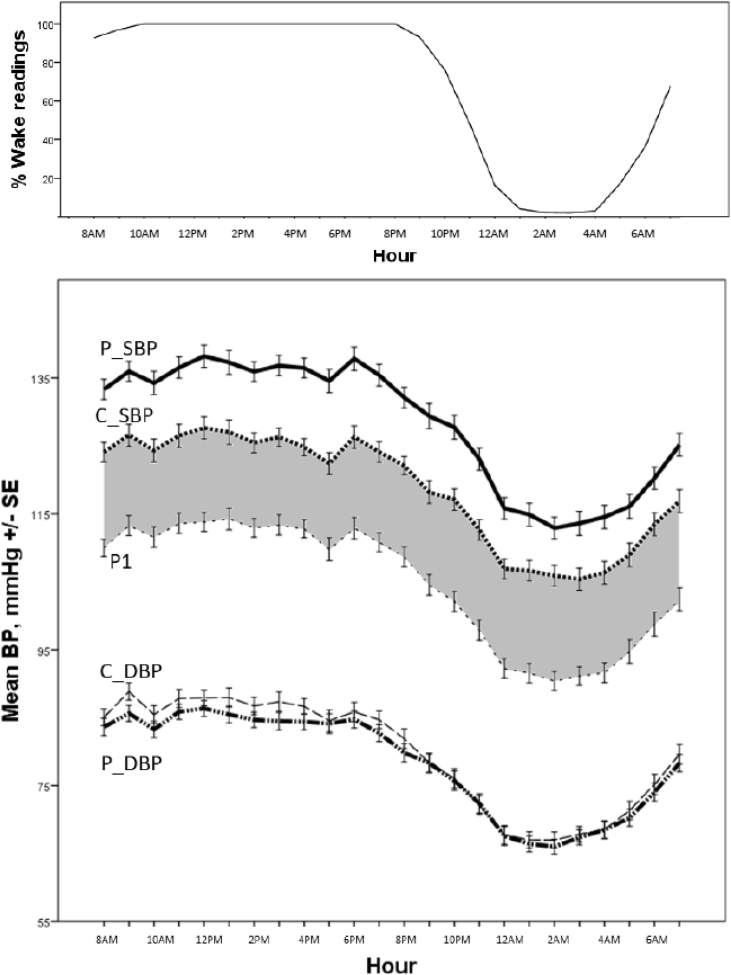
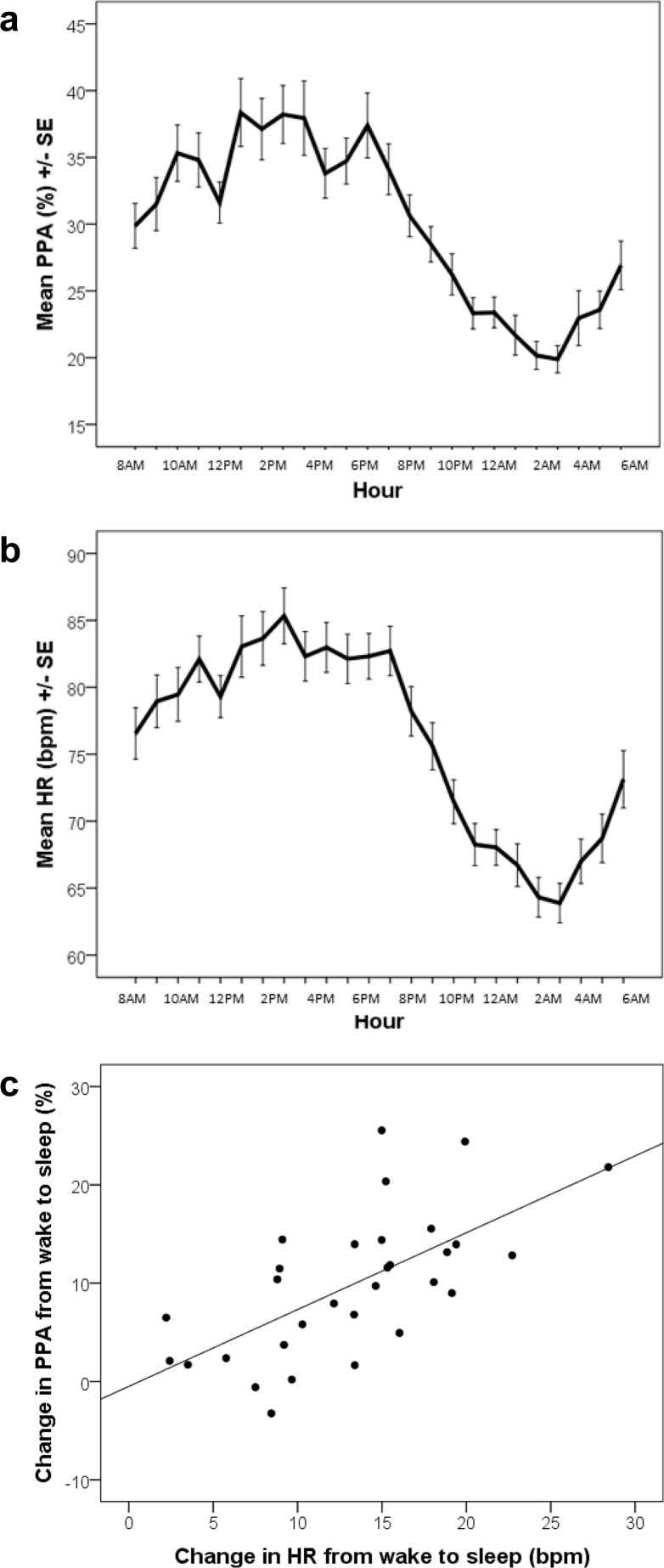
36 patients were screened, 31 had successful testing (mean (SD) age 45 ± 10 years, AHI 58 ± 27 events/hr, Office BP 136/89 ± 10.7/9.5 mmHg, 32% on anti-hypertensives, 77% dippers), 21 completed testing post CPAP. Central systolic and diastolic BP followed the same nocturnal dipping profile as peripheral BP, however the peripheral pulse pressure (PP) narrowed in sleep (−3.2 mmHg, p < 0.001), whereas the central PP remained unchanged (0.124 mmHg, NS), causing a significant reduction in PPA overnight (−10.7%, p < 0.001). The magnitude of dip in central systolic pressure was less than peripheral systolic pressure (by 2.3 mmHg, p < 0.001). After treatment with CPAP, the PPA reduction overnight was attenuated (by −3.3%, p = 0.004).
Conclusions
In moderate to severe OSA, central BP and PPA reduce overnight during sleep. Further randomised controlled studies are needed to quantify the differential effects of CPAP and anti-hypertensives on central versus peripheral BP.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
