Biggie Baffour-Awuah , Gudrun Dieberg , Melissa J. Pearson , Neil A. Smart
{"title":"Blood pressure control in older adults with hypertension: A systematic review with meta-analysis and meta-regression","authors":"Biggie Baffour-Awuah , Gudrun Dieberg , Melissa J. Pearson , Neil A. Smart","doi":"10.1016/j.ijchy.2020.100040","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Managing blood pressure reduces CVD risk, but optimal treatment thresholds remain unclear as it is a balancing act to avoid hypotension-related adverse events.</p></div><div><h3>Objectives</h3><p>This systematic review, meta-analysis and meta-regression evaluated the benefits of intensive BP treatment in hypertensive older adults.</p></div><div><h3>Methods</h3><p>We systematically searched PubMed, MEDLINE, EMBASE, and the Cochrane Library of Controlled Trials until January 31, 2020. Studies comparing different BP treatments/targets and/or active BP against placebo treatment, with a minimum 12 months follow-up, were included. Risk ratios (RR) and 95% CIs were calculated using a random effects model. The primary outcome was RR of major cardiovascular events (MCEs); secondary outcomes included myocardial infarction (MI), stroke, heart failure (HF), cardiovascular (CV) mortality, and all-cause mortality.</p></div><div><h3>Results</h3><p>We included 16 studies totaling 65,890 hypertensive participants (average age 69.4 years) with a follow-up period from 1.8 to 4.9 years. Intensive BP treatment significantly reduced the relative risk of MCEs by 26% (RR:0.74, 95%CI 0.64–0.86, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 79.71%). RR of MI significantly reduced by 13% (RR:0.87, 95%CI 0.76–1.00, <em>p</em> = 0.052; <em>I</em><sup>2</sup> = 0.00%), stroke by 28% (RR:0.72, 95%CI 0.64–0.82, <em>p</em> = 0.000; <em>I</em><sup><em>2</em></sup> = 32.45%), HF by 47% (RR:0.53, 95% CI 0.43–0.66, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 1.23%), and CV mortality by 24% (RR:0.76, 95%CI 0.66–0.89, <em>p</em> = 0.000; <em>I</em><sup>2</sup> = 39.74%). All-cause mortality reduced by 17% (RR:0.83, 95%CI 0.73–0.93, <em>p</em> = 0.001; <em>I</em><sup>2</sup> = 53.09%). Of the participants - 61% reached BP targets and 5% withdrew; with 1 hypotension-related event per 780 people treated.</p></div><div><h3>Conclusions</h3><p>Lower BP treatment targets are optimal for CV protection, effective, well-tolerated and safe, and support the latest hypertension guidelines.</p></div>","PeriodicalId":36839,"journal":{"name":"International Journal of Cardiology: Hypertension","volume":"6 ","pages":"Article 100040"},"PeriodicalIF":0.0000,"publicationDate":"2020-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.ijchy.2020.100040","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Cardiology: Hypertension","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590086220300173","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/7/7 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 8
Abstract
Background
Managing blood pressure reduces CVD risk, but optimal treatment thresholds remain unclear as it is a balancing act to avoid hypotension-related adverse events.
Objectives
This systematic review, meta-analysis and meta-regression evaluated the benefits of intensive BP treatment in hypertensive older adults.
Methods
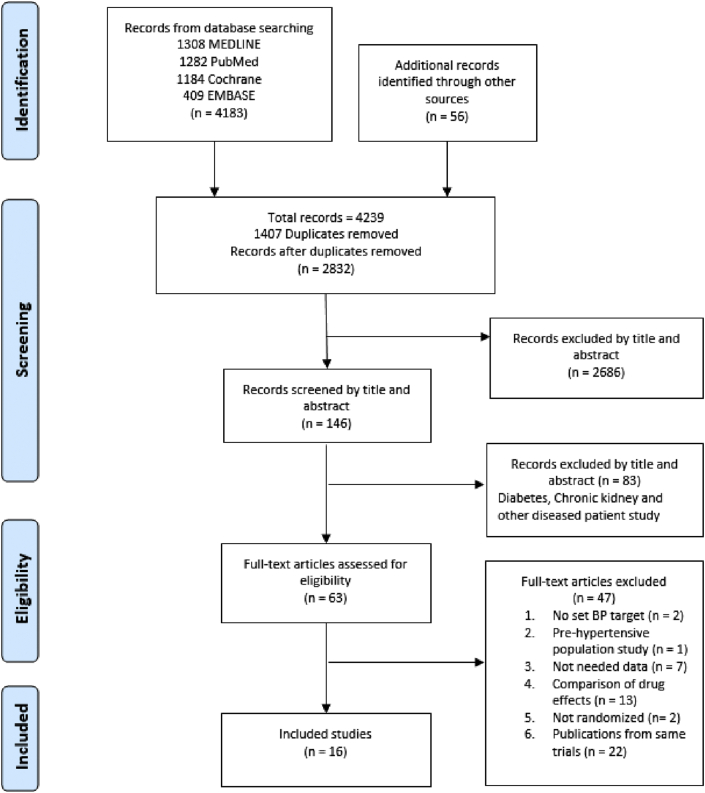
We systematically searched PubMed, MEDLINE, EMBASE, and the Cochrane Library of Controlled Trials until January 31, 2020. Studies comparing different BP treatments/targets and/or active BP against placebo treatment, with a minimum 12 months follow-up, were included. Risk ratios (RR) and 95% CIs were calculated using a random effects model. The primary outcome was RR of major cardiovascular events (MCEs); secondary outcomes included myocardial infarction (MI), stroke, heart failure (HF), cardiovascular (CV) mortality, and all-cause mortality.
Results
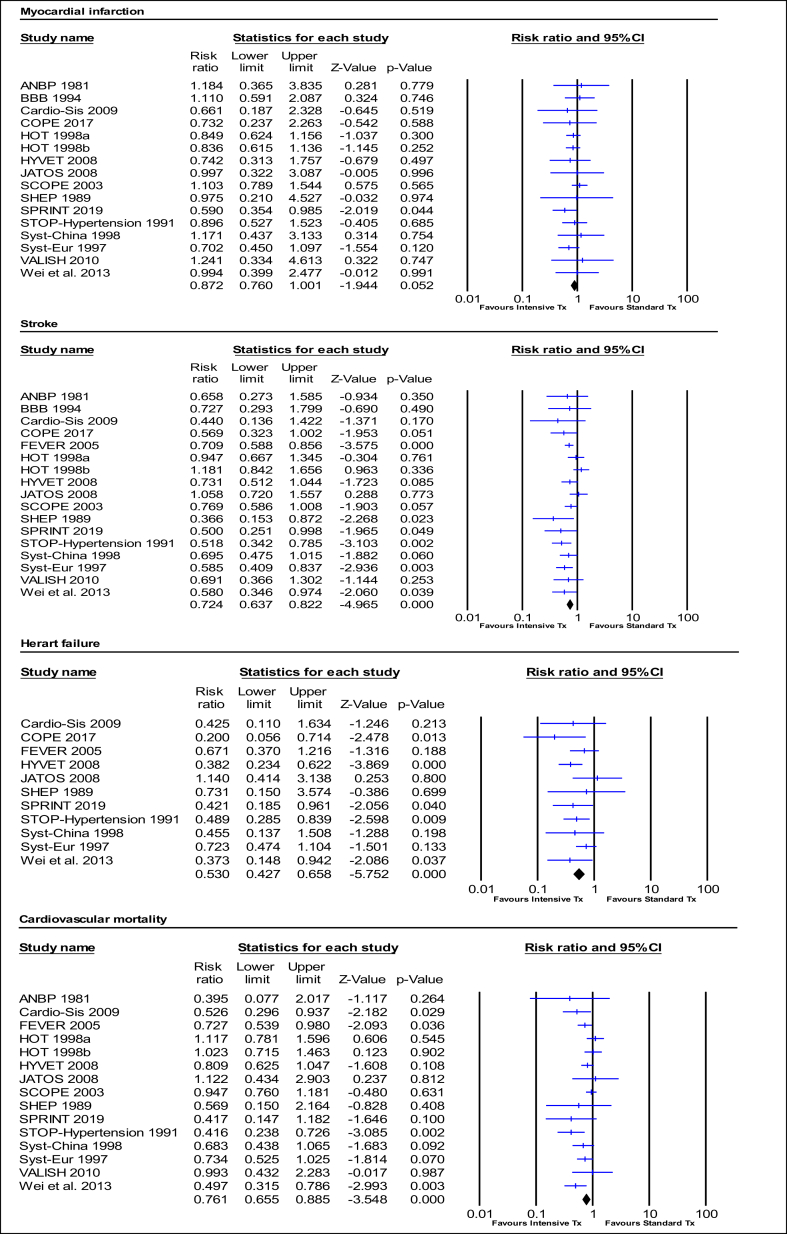
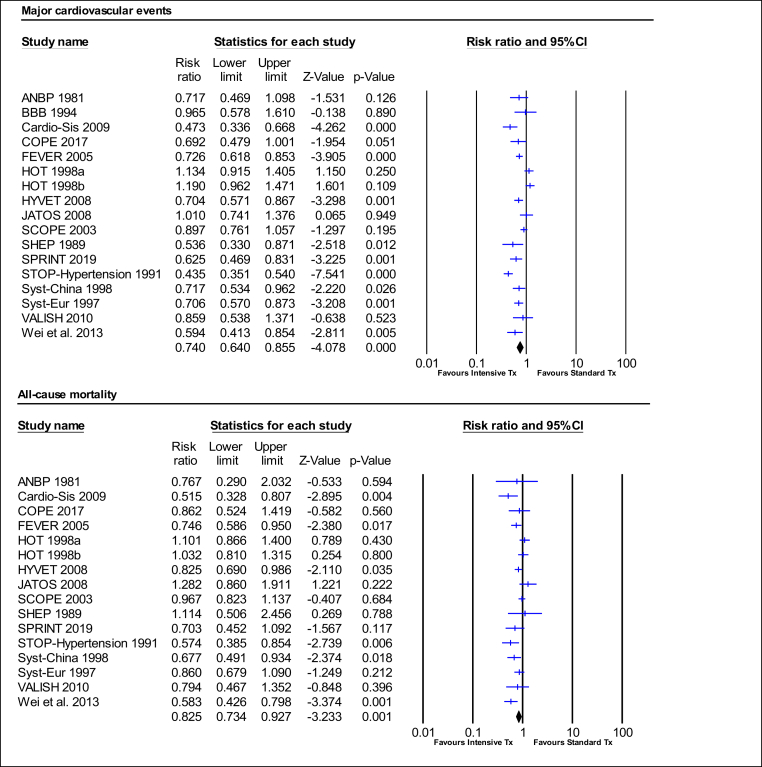
We included 16 studies totaling 65,890 hypertensive participants (average age 69.4 years) with a follow-up period from 1.8 to 4.9 years. Intensive BP treatment significantly reduced the relative risk of MCEs by 26% (RR:0.74, 95%CI 0.64–0.86, p = 0.000; I2 = 79.71%). RR of MI significantly reduced by 13% (RR:0.87, 95%CI 0.76–1.00, p = 0.052; I2 = 0.00%), stroke by 28% (RR:0.72, 95%CI 0.64–0.82, p = 0.000; I2 = 32.45%), HF by 47% (RR:0.53, 95% CI 0.43–0.66, p = 0.000; I2 = 1.23%), and CV mortality by 24% (RR:0.76, 95%CI 0.66–0.89, p = 0.000; I2 = 39.74%). All-cause mortality reduced by 17% (RR:0.83, 95%CI 0.73–0.93, p = 0.001; I2 = 53.09%). Of the participants - 61% reached BP targets and 5% withdrew; with 1 hypotension-related event per 780 people treated.
Conclusions
Lower BP treatment targets are optimal for CV protection, effective, well-tolerated and safe, and support the latest hypertension guidelines.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
