Justin E Hellwinkel, Matthew W Konigsberg, Johana Oviedo, Paula M Castaño, R Kumar Kadiyala
{"title":"Subfascial-located contraceptive devices requiring surgical removal.","authors":"Justin E Hellwinkel, Matthew W Konigsberg, Johana Oviedo, Paula M Castaño, R Kumar Kadiyala","doi":"10.1186/s40834-021-00158-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Subdermal etonogestrel implants are highly effective contraceptive methods. Despite standardization of insertion technique by the manufacturer, some implants are inadvertently placed too deeply within or below the plane of the biceps brachii fascia. Placement of these implants in a deep tissue plane results in more difficult removal, which is not always possible in the office setting. In rare cases, surgical removal by an upper extremity surgeon is warranted.</p><p><strong>Case presentation: </strong>Here we present 6 cases of etonogestrel implants located in a subfascial plane requiring removal by an upper extremity surgeon. Implants were all localized with plain radiography and ultrasound prior to surgical removal. All cases had implants located in the subfascial plane and one was identified intramuscularly. The average age was 28 years (19-33) and BMI was 24.0 kg/m^2 (19.1-36.5), with the most common reason for removal being irregular bleeding. The majority of cases (5/6) were performed under monitored anesthesia care with local anesthetic and one case utilized regional anesthesia. All implants were surgically removed without complication.</p><p><strong>Conclusions: </strong>Insertion of etonogestrel contraceptive implants deep to the biceps brachii fascia is a rare, but dangerous complication. Removal of these implants is not always successful in the office setting and referral to an upper extremity surgeon is necessary to avoid damage to delicate neurovascular structures for safe removal.</p>","PeriodicalId":10637,"journal":{"name":"Contraception and Reproductive Medicine","volume":"6 1","pages":"13"},"PeriodicalIF":0.0000,"publicationDate":"2021-05-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40834-021-00158-5","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception and Reproductive Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40834-021-00158-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: Subdermal etonogestrel implants are highly effective contraceptive methods. Despite standardization of insertion technique by the manufacturer, some implants are inadvertently placed too deeply within or below the plane of the biceps brachii fascia. Placement of these implants in a deep tissue plane results in more difficult removal, which is not always possible in the office setting. In rare cases, surgical removal by an upper extremity surgeon is warranted.
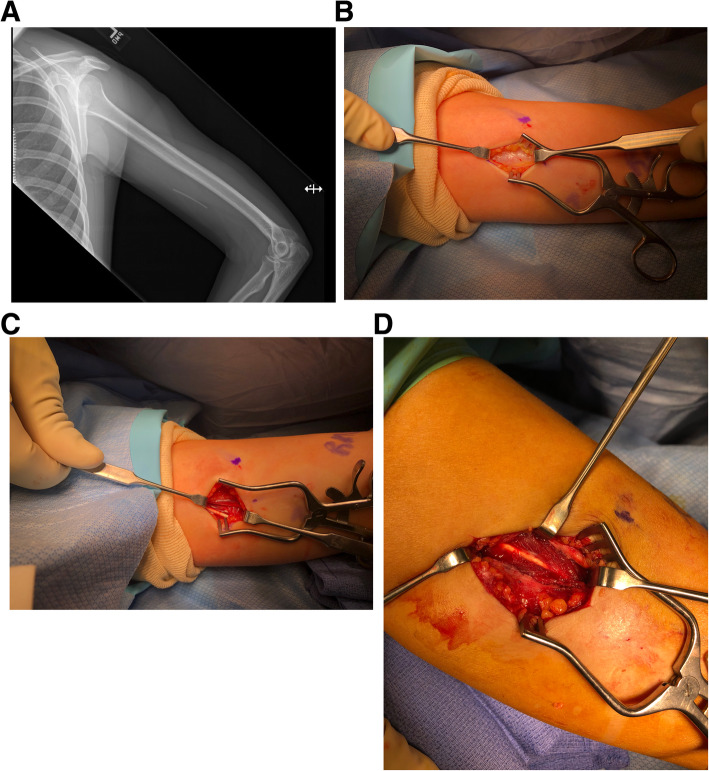
Case presentation: Here we present 6 cases of etonogestrel implants located in a subfascial plane requiring removal by an upper extremity surgeon. Implants were all localized with plain radiography and ultrasound prior to surgical removal. All cases had implants located in the subfascial plane and one was identified intramuscularly. The average age was 28 years (19-33) and BMI was 24.0 kg/m^2 (19.1-36.5), with the most common reason for removal being irregular bleeding. The majority of cases (5/6) were performed under monitored anesthesia care with local anesthetic and one case utilized regional anesthesia. All implants were surgically removed without complication.
Conclusions: Insertion of etonogestrel contraceptive implants deep to the biceps brachii fascia is a rare, but dangerous complication. Removal of these implants is not always successful in the office setting and referral to an upper extremity surgeon is necessary to avoid damage to delicate neurovascular structures for safe removal.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
