A retrospective cohort study comparing clinical outcomes and healthcare resource utilisation in patients undergoing surgery for osteomyelitis in England: a case for reorganising orthopaedic infection services.
Jamie Ferguson, Myriam Alexander, Stuart Bruce, Matthew O'Connell, Sue Beecroft, Martin McNally
{"title":"A retrospective cohort study comparing clinical outcomes and healthcare resource utilisation in patients undergoing surgery for osteomyelitis in England: a case for reorganising orthopaedic infection services.","authors":"Jamie Ferguson, Myriam Alexander, Stuart Bruce, Matthew O'Connell, Sue Beecroft, Martin McNally","doi":"10.5194/jbji-6-151-2021","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aims</b>: An investigation of the impact of a multidisciplinary bone infection unit (BIU) undertaking osteomyelitis surgery with a single-stage protocol on clinical outcomes and healthcare utilisation compared to national outcomes in England. <b>Patients and Methods</b>: A tertiary referral multidisciplinary BIU was compared to the rest of England (ROE) and a subset of the 10 next busiest centres based on osteomyelitis treatment episode volume (Top Ten), using the Hospital Episodes Statistics database (HES). A total of 25 006 patients undergoing osteomyelitis surgery between April 2013 and March 2017 were included. Data on secondary healthcare resource utilisation and clinical indicators were extracted for 24 months before and after surgery. <b>Results</b>: Patients treated at the BIU had higher orthopaedic healthcare utilisation in the 2 years prior to their index procedure, with more admissions ( <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001) and a mean length of stay (LOS) over 4 times longer than other groups (10.99 d, compared to 2.79 d for Top Ten and 2.46 d for the ROE, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001). During the index inpatient period, the BIU had fewer mean theatre visits (1.25) compared to the TT (1.98, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001) and the ROE (1.64, <math><mrow><mi>p</mi> <mo>=</mo></mrow> </math> 0.001). The index inpatient period was shorter in the BIU (11.84 d), 33.6 % less than the Top Ten (17.83 d, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001) and 29.9 % shorter than the ROE (16.88 d, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001). During follow-up, BIU patients underwent fewer osteomyelitis-related reoperations than Top Ten centres ( <math><mrow><mi>p</mi> <mo>=</mo></mrow> </math> 0.0139) and the ROE ( <math><mrow><mi>p</mi> <mo>=</mo></mrow> </math> 0.0137). Mortality was lower (4.71 %) compared to the Top Ten (20.06 %, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001) and the ROE (22.63 %, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001). The cumulative BIU total amputation rate was lower (6.47 %) compared to the Top Ten (15.96 %, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001) and the ROE (12.71 %, <math><mrow><mi>p</mi> <mo><</mo></mrow> </math> 0.001). Overall healthcare utilisation was lower in the BIU for all inpatient admissions, LOS, and Accident and Emergency (A&E) attendances. <b>Conclusion</b>: The benefits of managing osteomyelitis in a multi-disciplinary team (MDT) specialist setting included reduced hospital stays, lower reoperation rates for infection recurrence, improved survival, lower amputation rates, and lower overall healthcare utilisation. These results support the establishment of centrally funded multidisciplinary bone infection units that will improve patient outcomes and reduce healthcare utilisation.</p>","PeriodicalId":15271,"journal":{"name":"Journal of Bone and Joint Infection","volume":"6 5","pages":"151-163"},"PeriodicalIF":2.8000,"publicationDate":"2021-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8137857/pdf/","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Bone and Joint Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5194/jbji-6-151-2021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
引用次数: 11
Abstract
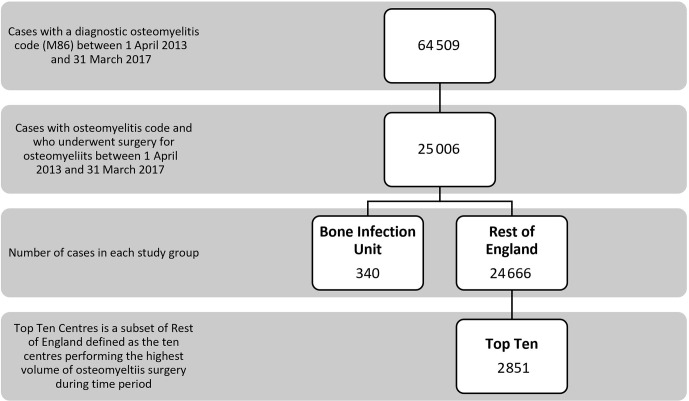
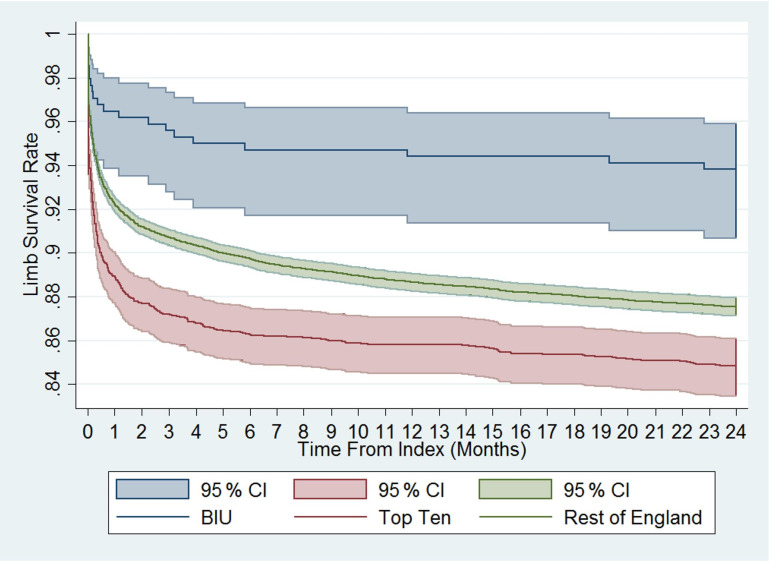
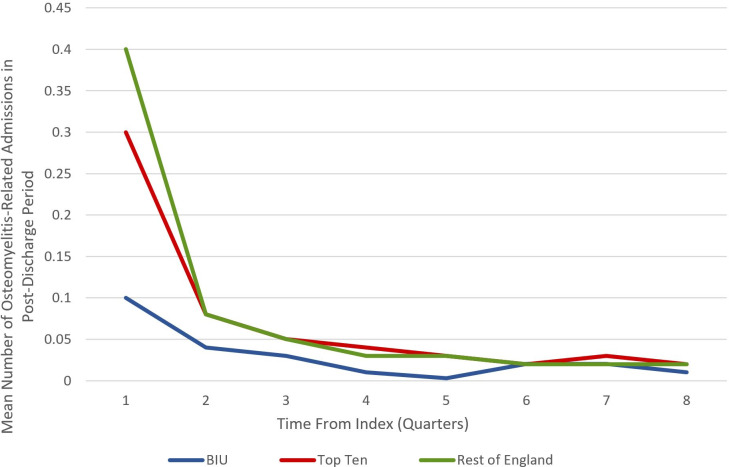
Aims: An investigation of the impact of a multidisciplinary bone infection unit (BIU) undertaking osteomyelitis surgery with a single-stage protocol on clinical outcomes and healthcare utilisation compared to national outcomes in England. Patients and Methods: A tertiary referral multidisciplinary BIU was compared to the rest of England (ROE) and a subset of the 10 next busiest centres based on osteomyelitis treatment episode volume (Top Ten), using the Hospital Episodes Statistics database (HES). A total of 25 006 patients undergoing osteomyelitis surgery between April 2013 and March 2017 were included. Data on secondary healthcare resource utilisation and clinical indicators were extracted for 24 months before and after surgery. Results: Patients treated at the BIU had higher orthopaedic healthcare utilisation in the 2 years prior to their index procedure, with more admissions ( 0.001) and a mean length of stay (LOS) over 4 times longer than other groups (10.99 d, compared to 2.79 d for Top Ten and 2.46 d for the ROE, 0.001). During the index inpatient period, the BIU had fewer mean theatre visits (1.25) compared to the TT (1.98, 0.001) and the ROE (1.64, 0.001). The index inpatient period was shorter in the BIU (11.84 d), 33.6 % less than the Top Ten (17.83 d, 0.001) and 29.9 % shorter than the ROE (16.88 d, 0.001). During follow-up, BIU patients underwent fewer osteomyelitis-related reoperations than Top Ten centres ( 0.0139) and the ROE ( 0.0137). Mortality was lower (4.71 %) compared to the Top Ten (20.06 %, 0.001) and the ROE (22.63 %, 0.001). The cumulative BIU total amputation rate was lower (6.47 %) compared to the Top Ten (15.96 %, 0.001) and the ROE (12.71 %, 0.001). Overall healthcare utilisation was lower in the BIU for all inpatient admissions, LOS, and Accident and Emergency (A&E) attendances. Conclusion: The benefits of managing osteomyelitis in a multi-disciplinary team (MDT) specialist setting included reduced hospital stays, lower reoperation rates for infection recurrence, improved survival, lower amputation rates, and lower overall healthcare utilisation. These results support the establishment of centrally funded multidisciplinary bone infection units that will improve patient outcomes and reduce healthcare utilisation.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
